 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
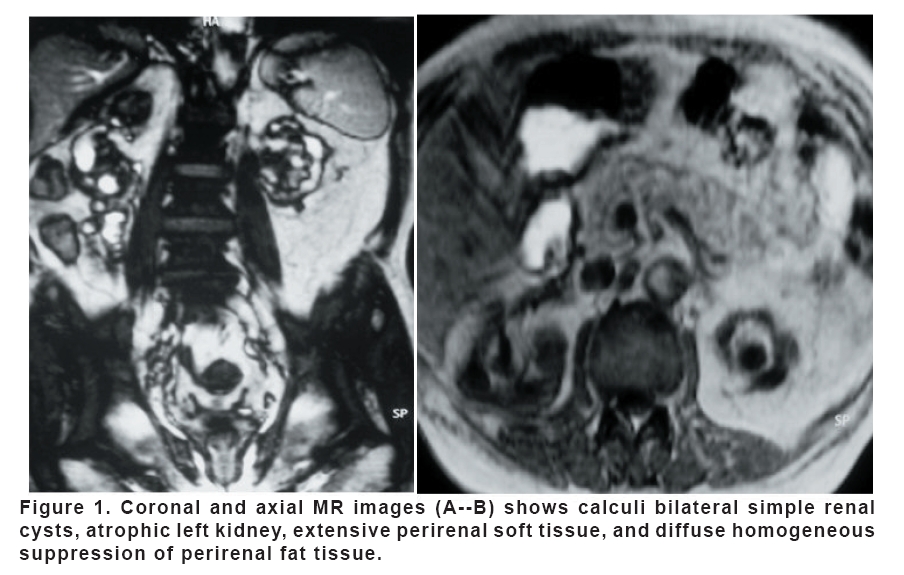
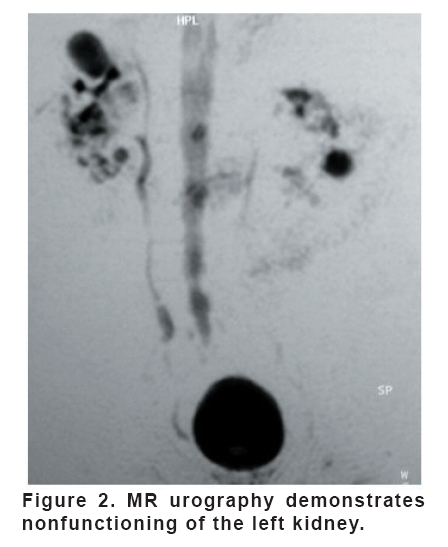
European Journal of General Medicine, Vol. 5, No. 3, 2008, pp. 184-186 Replacement Lipomatosis Of The Kidney: MRI Features Güner Sönmez1, Hakan Mutlu1 ,Ersin Özturk1,Onur Sıldıroğlu1, İlker Akyol2, C Çınar Başekim1, Eşref Kızılkaya1 Gulhane Military Medical Academy Haydarpasa Teaching Hospital, Department of Radiology1 and Urology2, İstanbul, Turkey. Code Number: gm08036 Renal replacement lipomatosis of the kidney is characterized by renal sinus and perirenal fat proliferation. It is associated with chronic infection and calculi, commonly central, often obstructing. The kidney may be large or small but is usually nonfunctioning. Most of the renal parenchyma has been replaced by fat, pararenal fascia are thickened, and there may be fistulae. We reported radiological findings of renal replacement lipomatosis in a 55 year-old man. Key words: Kidney, calculi, lipomatosis, MRI, CT, radiography INTRODUCTION Renal replacement lipomatosis (RRL) is a rare condition involving growth of fat within the renal sinus, hilum and perirenal space often associated with renal calculi. The pathogenesis of RRL is unknown, although it is generally associated with aging, renal atrophy, long-standing chronic urinary infections (1). There are no specific clinical symptoms indicating RRL. The patient may be asymptomatic or various symptoms related to the primary disease, the most frequent manifestions being urinary tract infections, flank pain, fever and mass. The clinical importance of RRL is that resemble fat-containing renal tumors. The diagnosis of RRL by US, CT and MRI can be difficult. CT of the urinary tract has gained popularity since the advent of helical CT. It requires injection of contrast material and is an irradiating method. Usefulness of MR imaging of the urinary tract was known and RRL depicted by MR imaging. CASE A 55-year-old man was admitted to our hospital complaining of left flank mass. He had a history of bilateral multiple renal calculi. He underwent radiography, US, CT and MRI studies. He has renal failure and hypertension. He had been using antihypertensive drugs for 10 years. An abdominal radiography showed bilateral multiple renal calculi. Renal sonography also showed multiple renal calculi associated with hyperechogenity araound left kidney. We could not make intravenous urography because of the renal failure. We obtained nonenhanced abdominopelvic CT for further evaluation. The CT scan through the upper kidneys revealed bilateral renal calculi and parenchymal atrophy with marked fatty proliferation within the left renal sinus, hilus, and perinephric space. We considered lipoma or low-grade liposarcoma as differential diagnoses. MR imaging was performed using a 1.5-T scanner with a phased array body coil. Patients were asked to void before MR urography examination. Otherwise, no specific preparation was required, and no external compression was applied. Breath-hold sequences were used. Both two-dimensional T2-weighted MR urography and 3D T1-weighted MR urography were performed in coronal orientation. T2-weighted MR urography was performed with thin-slice (fat-suppressed HASTE) and thick-slab (fat-suppressed heavily T2 turbo spin-echo) acquisitions. T1-weighted MR urography was performed with gadolinium-enhanced 3D FLASH acquisition. A low-dose diuretic injection of 0.1 mg/kg of body weight (total individual dose not exceeding 10 mg) of furosemide (Lasix) was used to enhance excretion 30-60 sec before the administration of contrast material. Three-dimensional FLASH sequences were routinely repeated 5 and 15 min after the administration of 0.1 mmol/kg of body weight of gadopentatate dimeglumine (Magnevist; Schering, Berlin, Germany). The patient was imaged supine, and the following MR imaging protocols were used: Heavily T2-weighted turbo spin-echo images was applied in coronal planes (TR/TE, 2800/1100; flip angle, 150°; matrix, 240x256; FOV, 450 mm; slab thickness, 60 mm). Coronal and axial GRE T1-weighted fat supressed sequence (TR/TE, 174.9/4.1 msec ; section thickness 5 mm; matrix 115x256; FOV 450 mm and acquisition time of 0.22 min), Trufi (TR/TE, 4.8/2.3 msec; slice thickness, 8 mm; FOV 500 mm; matrix; 192x256; acquisition time, 12 sec) and a gadolinium-enhanced breath-hold three-dimensional fast low-angle shot (3-D FLASH) acquisition (TR/TE, 4.6/1.8 msec; flip angle, 30°; effective slice thickness, 1.5 mm; FOV 342 mm; matrix; 192 × 256; acquisition time, 28 sec) were used. Postacquisition image processing was done on a remote console, using maximum intensity projection (MIP) to yield a three-dimensional urogram. Total imaging time of all MR sequences was approximately 25 minutes. MR images showed calculi, bilateral simple renal cysts, atrophic left kidney, extensive perirenal soft tissue, and diffuse homogeneous suppression of perirenal fat tissue (Figure 1). On MR urography, nonfunctioning of the left kidney was demonstrated (Figure 2). DISCUSSION RRL, also known as replacement lipomatosis is an advanced form of renal sinus lipomatosis that usually occurs unilaterally. A varying amount of fat and fibrous tissue is present within the renal sinus, hilus and perirenal areas. It may develop in obesity, Cushing’s syndrome or renal atrophy. And also use of exogenous steroids may cause renal lipomatosis (3,4). The severe loss of parenchyma with massive fat deposition is associated with inflammatory changes and calculi in 76-79% of cases (2). Associated nonspecific clinical symptoms are urinary tract infection, fever, flank pain, weight loss and hematuria. The renal cortex is extremely atrophied, with varying degrees of hydronephrosis or pyonephrosis. The major differential diagnosis in the presence of long standing inflammation and calculous obstruction is xantogranulomatous pyelonephritis. The attenuation of lipomatosis tissue may approach zero simulating a hydronephrosis, cyst, or myxoid liposarcoma if the fat/fibrous tissue ratio decreases. Fat containing neoplasms arising in the parenchyma, renal sinus, renal capsule, or perinephric space, such as angiomyolipoma, lipoma, and liposarcoma, can also be readily differentiated from RRL. In addition to the marked loss of renal parenchyma, nonfunctioning of the kidney, and renal calculi, the adipose tissue in RRL is concentrated to a location corresponding to the renal sinus and hilus possible with a diffuse extension perirenal space (2,5,6). Heavily T2-weighted pulse sequences to obtain static water images of the urinary tract. T2-weighted MR urograms have proved excellent in the visualization of the markedly obstructed collecting system, even if the renal excretory function is quiescent. T2-weighted MRU is less suitable for the imaging of abnormalities that occur in the nondilated urinary tract. The HASTE MR sequence is a breathing-independent T2–weighted spin-echo ultrafast sequence with great sensitivity for fluid detection. With it, breathing-related ghosting artifact, bowel motion, and magnetic susceptibly difference artifact from air and bowel are largely eliminated. It allows for differentiation of dilated ureter and distal ureter calculus without exogenous contrast. Neverthless, 3-D FLASH sequence, with its short acquisition time, permits repeated series of breath-hold images in optimal orientations, thus providing obvious improvement to the methods previously described by other investigators. The whole UT, including nondilated ureter, can be visualized. The high resolution images allow good reconstructed image quality. High quality MIP images and multiplanar reconstructions are of use especially in evaluating the distal ureter: MIP images resemble those of IVU, with better spatial resolution than HASTE sequence. Diffuse and homogenous suppression of perirenal fat tissue with fat suppression sequence is also useful in differentiation from tumors including fat and arising in the parenchyma, renal sinus, renal capsule, or perinephric space, such as angiomyolipoma, lipoma, and liposarcoma (5,6). In conclusion, MR imaging is a valuable imaging technique for examining patients with RRL. MR sequences can rapidly reveal the presence of perirenal fat intensity signal, obstruction, dilated ureter, level of obstruction, and atrophic kidney, and thus rapidly provide information for diagnosis this pathology. To our knowledge, this is only the second case in the literature describing the MRI findings of RRL. REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08036f1.jpg] [gm08036f2.jpg] |
| |||||||||

{kind=link}
{kind=link}