 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
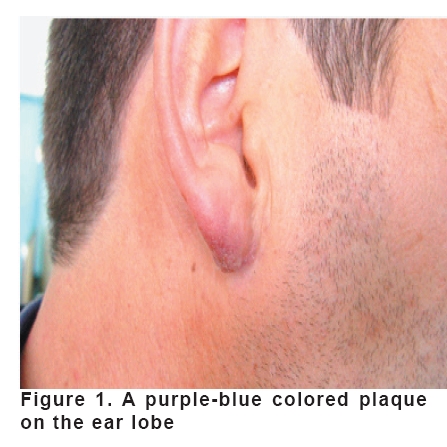
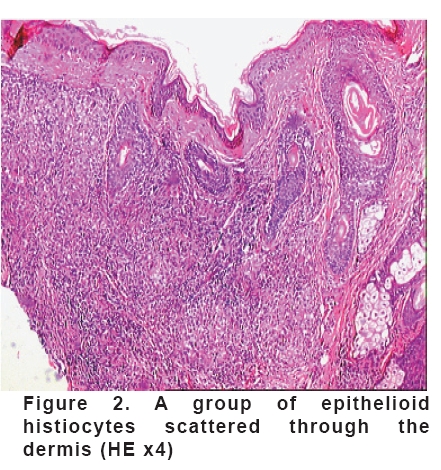
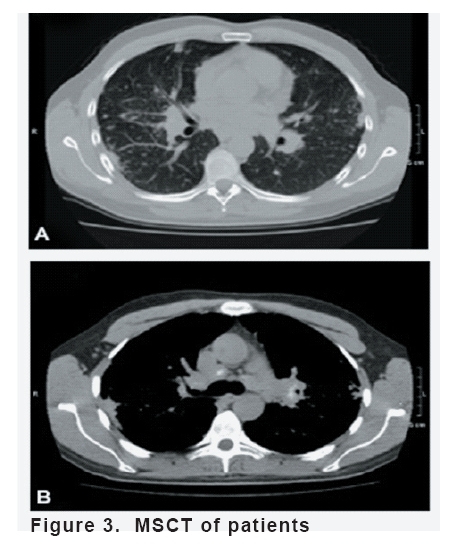
European Journal of General Medicine, Vol. 5, No. 3, 2008, pp. 191-193 Lupus Pernio On Ear Lobe That Occured After Trauma Cihangir Aliağaoğlu1, Mustafa Atasoy2, Mustafa Keleş3, Kerim Çayır3, Aysun Toker4 Numune State Hospital, Departments of Dermatology1 and Biochemistry4, Atatürk University, Faculty of Medicine, Departments of Internal Medicine2 and Dermatology3, Erzurum, Turkey Code Number: gm08038 In the present 35 years old male patient, there were lupus pernio plaque in the right ear lobe developed after blunt trauma and radiologically typical sarcoidosis findings. In histopatholigical examination, clusters of epithelioid cells scattered irregularly through the dermis were observed. The patient responded well to systemic and topical steroid therapy. Key words: Lupus pernio, trauma INTRODUCTION Sarcoidosis is a multisystem disease of unknown etiology characterized by the formation of noncaseating granulomas in the affected organs. Although different series report variable incidences of skin involvement during the course of the disease, nearly one-fourth of sarcoidosis patients have skin involvement (1). Lupus pernio (LP) was first described by Ernest Besnier in 1889 (2). The lesions are chronic and violaceous and are usually found on the nose, cheeks, ears and fingers. There may be associated plaques on the arms, buttocks, and thighs. It occurs more frequently in women. In one series of patients with LP, a close association was found with other forms of chronic fibrotic sarcoidosis, in particular, intrathoracic disease, upper respiratory tract involvement and the presence of bone cysts (2,3). Cutaneous sarcoidosis is known to occur at the sites of scar and trauma but LP has not been widely recognized to show this phenomenon (2). Although a case with LP developing after trauma to the nose has been reported in the literature (2), we could not meet any case report indicating the development of LP after trauma. Thus, we aimed to present such an interesting case. CASE A patient who had a blunt trauma (a fist to ear) to his ear 1 year ago and who had had a blue-purple eruption on the ear lobe for the last 6 months visited our clinic for this eruption. We learnt that the eruptions occurred on the side of his ear affected by the trauma. There was not anyone else who had this disease in his family. In dermatologic examination; there was a plaque lesion which was blue-purple in color, sharp sided and lighty porosized and the whole ear lobe was completely affected (Figure 1). The following investigations were in normal ranges; complete blood count, urea and electrolytes, liver function tests, serum calcium and phosphate, creatine, immunglobulins, serum angiotensin converting enzyme, 24-h urine calcium excretion, ECG and lung function tests. A Kveim test was positive. X-rays of hands showed normal findings. In histopathological examination; epithelioid histiocyte aggregates in various sizes, and rare lymphocytes were seen through dermis. There was an area which was not affected and was made by dermal collagens between epidermis and histiocyte aggregates (Figure 2). In multislice computed tomography (MSCT) axial imaging examination; pulmonary nodules which come together in paranchymal at bilateral pulmonary upper lobes and multiple lymph nodes in aorto-pulmonary window and upper mediastinum were seen (Figure 3). The patient was given topical steroid and 20mg/day prednisone perorally for 1.5 months. At the end of therapy, the lesion on the ear was nearly completely healed. No recurrence was seen on 2, 4 and 6 months follow ups. DISCUSSION Lesions of cutaneous sarcoidosis can also appear in preexisting scars. This condition is known as scar sarcoidosis (4). It often occurs in scars on the knees but may also arise in surgical scars or at injection and venepuncture sites (2). Sarcoidosis occuring in scars as a Koebner phenomenon is well documented and this may be the only manifestation of sarcoidosis (2). When the papules or plaques are situated on the nose, cheeks, and ears, the term lupus pernio is applied (5). The lesion in our case has occurred after trauma on normal skin. The isomorphic response of Koebner involves the development of lesions in previously normal skin that has been traumatized either by physical damage, infection or allergic reactions. Development of lupus pernio after trauma is not excessively rare in clinic practice but it is not commonly reported in the literature (2). It seems to be difficult to say whether or not this case displays a true Koebner phenomenon because of less number of reported cases in the literature. Correct diagnosing of sarcoidosis may be a challenge. Unfortunately, no single test can prove the diagnosis. Patients are diagnosed with sarcoidosis when a compatible picture is present, along with histologic evidence of noncaseating granulomas, and when other potential causes, such as infections, are included (4). Granulomas may be present only in the superficial dermis or they may extend through the whole thickness of the dermis or subcutis, depending on the type of cutaneous lesion (6). LP-type lesions show variously sized aggregates of epithelioid cells scattered irregularly through the dermis with occasional extension into the subcutaneous tissue. In subcutaneous nodules, epithelioid cell tubercles lie in the subcutaneous fat (5). We diagnosed the present case as LP by clinical appearance of the lesions, the radiological findings on chest MSCT and histopathological examination. The treatment of cutaneous sarcoidosis is often frustrating, because lesions may be refactory to treatment or may recur following successful treatment. For localized involvement, topical or intralesional steroids are used. Systemic agents are needed for widespread, progressive lesions or those that impair function. Systemic glucocorticoids are the most effective agents. They are commonly used at slow, tapering dosages, srarting at 20 to 40 mg of oral prednisone daily for six weeks. Many other medications may be used in refractory cases, including such agents as hydroxychloroquine, methotrexate, and thalidomide (1,4,7). CO2 laser excision is an alternative method to treat these lesions with excellent cosmetic results (3). In a recent study, successful results were obtained with the use of infliximab (8). We started peroral prednisolone (20mg/day) and topical steroid in the present case, and six weeks after the start of therapy, we observed that the lesions on the ear were nearly healed. REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08038f2.jpg] [gm08038f1.jpg] [gm08038f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}