 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
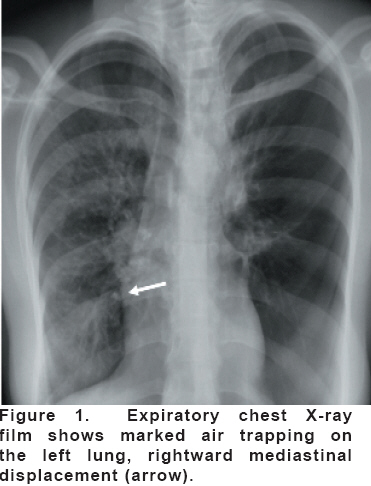
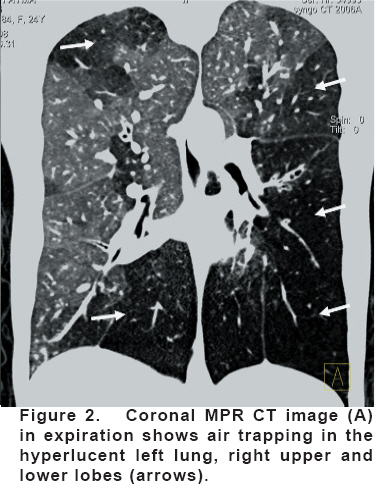
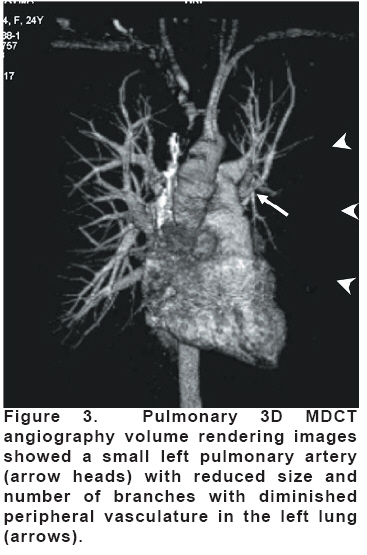
European Journal of General Medicine, Vol. 5, No. 3, 2008, pp. 194-197 Swyer–James Syndrome: Demonstration By 64-Slice 3D MDCT Angiography And Coronal MPR CT Imaging M.Emin Sakarya1, Osman Koç1, Olgun Arıbaş2, Orhan Özbek1, Yahya Paksoy1, Alaaddin Nayman1, Kemal Ödev1 Selcuk University, Faculty of Medicine, Departments of Radiology1 and Thoracic Surgery2, Konya, Turkey Code Number: gm08039 The 64-slice three dimensional (3D) multidetector computed tomography (MDCT) angiography and high resolution coronal multiplanar reformation (MPR) computed tomography (CT) images in inspiration and expiration were performed in a patient suspected of having Swyer – James syndrome. The right pulmonary system was normal. The left lung was small and hyperlucent. The left pulmonary arterial system was small but patent. Both lung contained bronchiectasis. High resolution coronal MPR CT images confirmed air trapping in the left lung and the right upper lobe. A diagnosis of Swyer-James syndrome was made. Key words: Lung, Multi-slice helical CT, Swyer – James syndrome INTRODUCTION Swyer – James syndrome (SJS) was first described by Swyer and James in a 6-year-old child in 1953 (1). The following year, MacLeod reported nine patients with unilateral pulmonary hyperlucency (2). SJS is a rare disease characterized by a hyperlucent lung or lobe, usually of normal or small size, associated with air trapping and diminutive pulmonary vascularization (3). Swyer-James syndrome appears to be a consequence of bronchiolitis obliterans resulting from bacterial or viral infection during childhood, which results in subsequent underdevelopment of the involved portion of the lung (4,5). Computed tomography (CT) by its ability to show bronchial patency, parenchymal lesions, and diminutive vascularization has been advocated as a valuable noninvasive modality in confirming the diagnosis of SJS (6,7). The multidetector computed tomography (MDCT) is considered a dramatic development in CT imaging that has direct implications in the three dimensional (3D) imaging of various systems, in particular the vascular system. The advantages of MDCT are an enormous increase in imaging acquisition speed, more coverage of the patient, and high spatial resolution (8). This technique combines the advantages of CT and angiography and allows a precise evaluation of the vascular, bronchial, and parenchymal structures especially, additional high resolution coronal multiplanar reformation (MPR) CT images are obtained in inspiration and expiration. In this case report, we presented the findings of 3D MDCT angiography and inspiratory and expiratory high resolution coronal MPR CT images in the evaluation of a patient with SJS. We report, to our knowledge, the first case of SJS documented by 3D MDCT angiography in this article. CASE A 24-year-old woman complained of dyspnea and productive cough. Laboratory data included a white blood cell count of 12,400/mm3. Electrocardiogram was normal. A chest radiograph obtained in inspiration showed a hyperlucent left lung (Figure 1). During expiration, the mediastinum moved to the right and the left hemidiaphragm remained immobile. 3D MDCT angiography was performed with a 64-slice scanner (Siemens Sensation 64, Erlangen, Germany). One hundred milliliters of iodinated contrast medium (100 ml of Ultravist, Germany) was injected at a rate of 4 ml/s, and after a delay of 15 s, a multislice acquisition was obtained from the aortic arch to the pulmonary basis with a scan time of 12 s, a slice thickness of 1 mm, a 1 mm interval between slices, and a matrix of 512 × 512. The volume rendering and maximum intensity projection (MIP) techniques were used. All the segmental pulmonary arteries and bronchi were identified by 3D MDCT angiography. Once thromboembolism was ruled out. The right pulmonary arterial system was patent and of normal size. The pulmonary artery and its branches were smaller on the left than on the right. Coronal MPR CT images obtained in expiration showed air trapping in the hyperlucent left lung, right upper and lower lobes (Figure 2). The left lower lobe and right middle lobe were contained severe bronchiectasis at axial CT images. Pulmonary 3D MDCT angiography volume rendering images showed a small pulmonary artery with reduced size and number of branches with diminished peripheral vasculature (Figure 3). A diagnosis of SJS, associated severe bronchiectasis, was made. DISCUSSION SJS is believed to be due to a lower tract infection in childhood with bronchiolitis obliterans (BO) resulting in peripheral air trapping and ultimately in destructive changes characteristic of emphysema (3). Bronchiectasis, probably secondary to recurrent infections, may develop proximal to BO (9). On the other hand, pathologic specimens from patients with bronchiectasis have shown associated BO. It is unclear whether BO occurs early in the pathogenesis of bronchiectasis or as a consequence of chronic suppuration in proximal dilated bronchi (10). Because the condition is usually acquired in childhood before the lungs have reached full development, the affected lung or lobe is usually small with reduced number of alveoli and subsequently hypodevelopment of the pulmonary arteries (11). The diagnosis of SJS is usually made on the basis of radiographic findings of hyperlucency of a lung or lobe, which results from air trapping during expiration and decreased pulmonary vascular markings in the involved area (6,7,12,13). Conventional pulmonary angiography has been described as the diagnostic standard (3). Because of its less invasive nature, dynamic bolus spiral CT angiography or MDCT angiography can be good alternative diagnostic tools, as compared with conventional angiography. There are two main differences between spiral CT and MDCT. Firstly, MDCT has a high acquisition speed; secondly, and probably more importantly, MDCT acquires volume data instead of individual slice data. These two factors together with thin section slices enable the new technique to provide almost isotropic data that can be arranged in different planes without compromising the spatial resolution of the original axial images (8). The MDCT makes it possible to examine the entire lung with thin slices during optimal enhancement in a single breath hold, allowing better depiction of the pulmonary vascular tree (14). In this case, the diagnosis was made with the 64-slice 3D MDCT angiography during bolus injection. The 3D MDCT angiography successfully depicted the small left pulmonary artery with a reduced number and size of branches with diminished peripheral vasculature in the left lung of the patient. In the 3D MDCT angiography, both pulmonary arteries and veins are enhanced with the contrast agent, and thus the reviewer must be careful to distinguish them. MDCT angiography is a rapidly evolving technique in the imaging of the pulmonary vasculature. The main disadvantages of MDCT angiography are the limited access to suitable MDCT technology. In this case, the 3D MDCT angiography combined with inspiratory and expiratory high resolution coronal MPR CT images allowed a complete evaluation of SJS. Inspiratory and expiratory high resolution coronal MPR CT images allowed evaluation of the parenchymal lesions. Expiratory high resolution coronal MPR CT images showed air trapping in the left lung, right lower and upper lobe. Contralateral lung involvement was identified. Both lung, left lower lobe and right middle lobe, were contained severe bronchiectasis. The result of this case suggests strongly that pulmonary 3D MDCT angiography in SJS is feasible, can depict the pulmonary vasculature in encouraging detail. The 3D MDCT angiography successfully showed pulmonary arterial branches with confidence in SJS. In conclusion, this case report indicates that the pulmonary 3D MDCT angiography is a fast and accurate technique for delineation of the main pulmonary artery and branches in patients with SJS and can be considered a noninvasive alternative to conventional angiography. The small pulmonary artery with a reduced number and size of branches with diminished peripheral vasculature can be visualized clearly with 3D MDCT angiography. The pulmonary 3D MDCT angiography and expiratory high resolution coronal MPR CT techniques might be considered to be a sensitive tool in patients with suspected SJS. REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08039f2.jpg] [gm08039f3.jpg] [gm08039f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}