 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
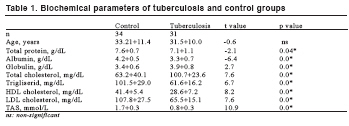
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 208-211 Assessment Of Antioxidants And Nutritional Status Of Pulmonary Tuberculosis Patients In Nigeria Akiibinu O Moses1, Ogunyemi O Emmanuel1, Arinola O Ganiyu2, Adenaike A Fidelis1, Adegoke O Dickson1* Olabisi Onabanjo University, Obafemi Awolowo College of Health Sciences, 1Department of Chemical Pathology and Immunology, Ago-Iwoye, Ogun state, University of Ibadan, 2Department of Chemical Pathology, Immunology unit, Ibadan Code Number: gm08041 Aim: The aim of this study was to assess the nutritional and antioxidant status of pulmonary tuberculosis patients in Nigeria Key words: Pulmonary tuberculosis, antioxidants, nutritional status, Nigeria. INTRODUCTION Tuberculosis is a highly infectious disease that is widely distributed throughout the world. The disease is influenced by economic and nutritional factors, although educational background, immunity and hormonal status have been associated with the prevalence (1,2). The economic and nutritional factors make the developing countries have the highest prevalent rate. The most popular causative agent is Mycobacterium tuberculosis although, Mycobacterium bovis, which affects cattles, can also be found in man (3). It is commonly a disease of the lungs (pulmonary tuberculosis) where it forms a localized infection after inhalation (4,1). It can affect extra pulmonary regions like lymph nodes, bone and joints, subcutaneous, meninges, eyes, the kidneys, and also the gastro-intestinal tract, where it causes an insidious disease that develops without any striking clinical evidence (5). It can also cause congenital tuberculosis transmissible from an infected mother to fetus following ingestion of the amniotic fluid containing Mycobacterium tuberculosis (6). The mycobacteria activate the invaded macrophages resulting to free radical burst (7,8). High serum levels of these free radicals and high lipid peroxidation products are characterized by patients with advanced tuberculosis (9). The peroxidation could cause reduced concentration of serum lipids and tissue inflammation (10). Study also stressed that apart from tissue inflammation and oxidative stress observed in these patients, tuberculosis also leads to continuous production of these free radicals that may cause a resultant low level of antioxidant (7). Tuberculosis has been associated with malnutrition. Yamanaka et al (11) reported that serum cholesterol was significantly lower in tuberculosis patients and got worse in homeless patients who were prone to starvation. The available reports on the assessment of free radical load, antioxidants and lipid peroxidation products only dealt with non- Nigerians tuberculosis patients. This study is also necessary in Nigeria, since these nutritional and metabolic derangements could contribute to the complications and low success rate in the treatment associated with pulmonary tuberculosis. Therefore, the present work was designed to investigate the plasma levels of TP, ALB, TG, TC, HDLC, LDLC, and total antioxidants in pulmonary tuberculosis infection. MATERIAL AND METHODS Thirty-one subjects with active tuberculosis and were sputum smear- positive volunteered to participate in this study. The radiological examination also showed pulmonary inflammation. Patients suffering from other pulmonary diseases were excluded from this study. Thirty-four apparently healthy sputum smear-negative individuals selected from staffs of State Hospital Adeoyo Ring road, Ibadan, Nigeria served as controls. Ten milliliters (10ml) of blood was collected from these subjects into a lithium heparin container and spun within one hour. The plasma sample for total antioxidants, lipid profiles, total protein, and albumin estimations were stored at –20oC until ready for analysis. Total antioxidant was measured using a standardized solution of Fe-EDTA complex that reacts with hydrogen peroxide to release a thiobarbituric reactive substance (12). Total protein was determined spectrophotometrically using alkaline solution of copper sulphate (13) , The albumin concentration was determined by the brilliant cresol green solution supplied by Dialab Production and Vertrieb vonchemich-technischen, Wien- Panikengasse , The globulin (GLOB) level was calculated by substracting the value of albumin from that of total protein. TC, HDLC, LDLC and TG were measured spectrophotometrically using commercially prepared reagents purchased from Randox Laboratory ltd, UK. Statistical analysis The results were expressed as mean + S.D. Comparison was made using student t-test while p<0.05 was regarded as significant. RESULTS In table 1, there was no significant difference in the age range (p>0.05) of patients with tuberculosis when compared with the controls selected for this study. The mean levels of TP (7.13+1.06g/dl), and ALB (3.27+0.7g/dl) were significantly lower in tuberculosis patients while the level of GLOB (3.9+0.84g/dl) was significantly higher when tuberculosis patients were compared with controls (TP= 7.6+0.7g/dl; ALB= 4.2+0.48g/dl; GLOB= 3.4+0.6g/dl respectively). TC (100.7+23.6mg/dl), HDLC (28.6+7.2mg/dl), LDLC (65.5+15.1mg/dl), TG (61.6+16.2mg/dl) and TAS (0.83+0.34 mmol/l) were significantly lower in tuberculosis patients when compared with the controls (TC=163.2+40.1mg/dl; HDLC= 41.4+5.4mg/dl; LDLC= 107.8+27.5mg/dl; TG= 101.5+29.6mg/dl; TAS= 1.65+0.26mmol/l). DISCUSSION The present study shows significantly lower levels of total protein and albumin in subjects with pulmonary tuberculosis. Similar report was given by Sasaki et al (10), that albumin and total protein were significantly lower in pulmonary tuberculosis. Yamanaka et al (11) reported that the total protein, albumin, cholinesterase, hemoglobin and lymphocyte were significantly lower in homeless patients when compared with non-homeless tuberculosis patients and healthy men. Aily et al (14) also observed lower levels of albumin and heamatocrite in tuberculosis. Lower levels of total protein and albumin in this study might have been caused by anorexia, malnutrition and mal-absorption commonly observed in tuberculosis. Albumin is an important component of plasma antioxidant activity that primarily binds free fatty acids, divalent cations and hydrogen oxochloride (HOCI) (15). It is a negative acute phase protein which the plasma value decreases during infection, injury or stress possibly as a result of increased metabolic need for tissue repair and free radical neutralization. The free radicals attack the cell membrane causing tissue damage and wasting disease in pulmonary tuberculosis patients with resultant high level of uric acid (a powerful antioxidant). The uric acid is endogenously produced as a compensatory mechanism for the neutralization of free radicals (16). The lower level of albumin may therefore be one of the complications associated with pulmonary tuberculosis Significantly high level of globulin observed in tuberculosis in our study might have arisen from combination of elevation of different globulin fractions previously observed. Arinola and Igbi (17) reported high levels of IgG and IgM in pulmonary tuberculosis. Nagayama et al (18) also stated that hyperglobulinaemia in tuberculosis is one of the predictive factors for the development of residual pleural thickening in tuberculous pleurisy. Gatner et al (19) reported higher levels of alpha-I-antitrypsin in pulmonary tuberculosis patients. The high level of globulin observed in this study support the fact that humoral immune response is less affected and raises the possibility of polyclonal B cell activation in tuberculosis patients. Lower levels of TC, TG, LDLC and HDLC were observed in this study. Kwiatkowska et al (9) and Reddy et al, (20) have reported high levels of lipid peroxidation in all categories of pulmonary tuberculosis patients, irrespective of treatment status and this might have caused reduction in the concentration of serum lipids as observed in our study. It was shown that total cholesterol was significantly lower in tuberculosis patients when compared with pulmonary tuberculosis-free controls (10, 11). Triglycerides and LDLcholesterol are the chief constituents of cell membranes (21), while the HDL cholesterol protects the arterial walls of the blood circulatory system (22). Lower levels of lipids noticed in these patients could be a factor that predisposes them to cell and tissue damage, cardiovascular problems and low cellular immunity (23, 24). The lower levels of total cholesterol, HDLC, LDLC and TG observed in this study could be the result of impaired rate of lipid production and enhanced lipid catabolic rate associated with tuberculosis. Some previous workers have reported significantly low levels of total antioxidants, Zn and beta-carotene in pulmonary tuberculosis (7, 25). It was also reported that significantly lower levels of vitamin E and A were common in tuberculosis patients than in healthy Ethiopians (26). In our study, lower levels of total antioxidant were observed in pulmonary tuberculosis patients. This might be due to malnutrition and exhaustion in attempt to neutralize heavy load of free radicals in these patients. The result of this study shows lower levels of antioxidants and nutritional profiles in pulmonary tuberculosis patients. This could be associated with heavy load of free radicals, oxidative stress and lipid peroxidation. Improved nutrition and supplementation with antioxidant therapy in the treatment of pulmonary tuberculosis may prevent the oxidative stress and further complications. REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08041t1.jpg] |
| |||||||||

{kind=link}