 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
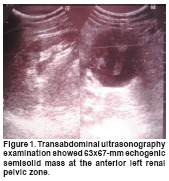
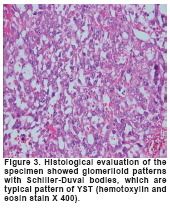
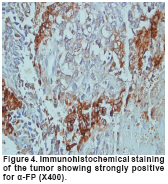
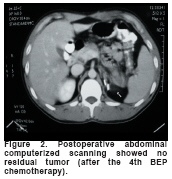
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 239-241 Primary Extragonadal Retroperitoneal Pure Yolk Sac Tumor Ömer Bayrak1, Ömer Faruk Karataş1, Reyhan Bayrak2 , Ersin Çimentepe1, Doğan Ünal1, Nuri Deniz3 Fatih University, School of Medicine, Departments of Urology1 and Pathology2, Gazi University, School of Medicine, Department of Urology3, Ankara, Turkey Code Number: gm08047 We describe a rare case of an extragonadal retroperitoneal pure yolk sac (endodermal sinus) tumor in the paraaortic region. Radiologic investigation, which included abdominal ultrasound ,computed tomography (CT), and magnetic resonance imaging (MRI) showed a large soft tissue mass occupying the inter paraaortic, renal, pancreatic and splenic region. Radionuclide bone scans demonstrated no bone metastases. The serum alpha fetoprotein (α-FP) level was high; however β-HCG was normal. Pathologic examination of the surgical specimen showed extragonadal yolk sac tumor. After postoperative chemotherapy, follow-up CT revealed decreased residual tumoral tissues and α-FP level returned to normal. Key words: Yolk sac tumor, retroperitoneal localization, extragonadal germ cell tumor INTRODUCTION Primary germ cell tumors of extragonadal origin are rare and exact incidence of this type cancer is unknown. They have been estimated to represent 3-5% of all adult germ cell malignancies (1). The origin of primary extragonadal germ cell tumors (EGGCT) is still a matter of debate. According to widely accepted theory, during embryogenesis, germ cells are misplaced anywhere at the midline. The mechanism of this misplacement is poorly understood, but malignant transformation of these cells leads to EGGCT at these regions (2-3). The most common sites of origin are, in decreasing order of frequency, the mediastineum, retroperitoneum, sacrococcygeal region and pineal gland, although many unusual sources have been reported (4). We report a case of primary extragonadal retroperitoneal pure Yolk sac tumor (YST) which could not be totally removed during operation and clinical remission was obtained after 4 courses of BEP chemotherapy. CASE A 27-year-old adult male was admitted to our department with the symptoms of bilateral inguinal pain. His past medical history was unremarkable and he had no urologic problems. No abnormality was observed during physical and genital examination. The abdominal ultrasonography revealed minimal left pelvicaliceal dilatation, 63x67-mm echogenic semisolid mass at the anterior left renal pelvic zone (Figure 1). The abdominal MRI showed large retroperitoneal tumor 7x7x6 cm in size (We can not show the preoperative CT and MR images due to the problem in our archive.) The tumoral mass was localized among the tail of the pancreas, spleen, left kidney and aorta. The tumor displaced the aortic wall medially and the tail of the pancreas superiorly. The mass was leading towards retroaortic region medially. The fatty tissues between the mass and kidney were diminished. The serum α-FP level was high (3537IU/ml, normal 1-7IU), β-HCG was normal (4.40-mIU/ml, normal 0-5 mIU/ml.). No echogenic pathology was obtained during scrotal ultrasonography. Extensive examination for metastases including Chest X-ray, chest CT, radionuclide bone scans demonstrated no abnormalities. The operation in September 2005 consisted of partial resection of the mass with the left kidney and the hiler–paraaortik lymph node dissection. Frozen biopsy of the tumor showed the typical pattern of the malign tumor. Histopathological evaluation of the specimen revealed an YST containing glomeriloid patterns with Schiller-Duval bodies, which are typical patterns of YST (Figure 3). Special immunohistochemical staining of the tumor was strongly positive for α-FP (Figure 4). On the postoperative 14th day, four courses of chemotherapy, consisting of BEP (bleomycin, etoposide, cisplatin) were administrated every 3 weeks to the patient. Serum α-FP level has fallen to normal range 18 weeks after the surgery. During the chemotherapy, follow-up CT showed a decrease in residual tumoral tissues (Figure 2). DISCUSSION Extragonadal germ cell tumors (EGGCT) are estimated to represent 3-5% of all germ cell malignancies (1). In adults these tumors most commonly arise in the midline of the mediastinum or the retroperitoneum (2-3). During the past two decades these cancers have become the model of curable neoplasm. The main reason is that these types of tumors are highly sensitive for cisplatinum-based chemotherapy protocols. Besides, new surgical, radiotherapatic and chemotheropatic treatment regimens have been described (5). The majority of adults with EGGCT present with advanced local disease and distant metastases, therefore complete local excision is rarely feasible. This tumor most commonly spread to the regional lymph nodes lung, liver and bone. Extragonadal germ cell tumors may reach a large size with no or relatively few symptoms. Patient with primary retroperitoneal tumors may present with abdominal or back pain, other vague constitutional symptoms, palpable mass or vascular obstruction (6). Our patient is in intermediate risk group according to International Germ Cell Cancer Collaborative Group (IGCCCG) classification (7). Many authors treat this group of patients with four courses of BEP chemotherapy first and then perform surgical resection (8). We explained the therapy alternatives to our patient and performed surgical excision before chemotherapy in the direction of the patient’s decision. The renal veins were surrounded by the tumor and the tumoral tissue could not be dissected from the kidney. Therefore, we performed nephrectomy, partial resection of the tumor and hilar-paraaortic lymph node resection. For the residual tumoral tissue, four courses of BEP chemotherapy were administrated. The patient responded very well to this therapy. Four months after surgery, total remission was achieved clinically, radiologically and biochemically. Total remission has been going on thirty months after the combination therapy (surgical excision and chemotherapy). As a result; in a case of a young male presenting with a retroperitoneal mass, EGGCTs should be taken into consideration in the differential diagnosis, because these tumors can be successfully treated by surgery and BEP chemotherapy like our patient with primary retroperitoneal pure YST. REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08047f1.jpg] [gm08047f4.jpg] [gm08047f2.jpg] [gm08047f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}