 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
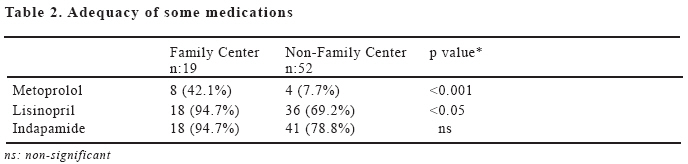
European Journal of General Medicine, Vol. 6, No. 1, 2009, pp. 11-14 Limited Availability of Anti-Hypertensive Medications in Primary Care in Kuwait Badria M. AL-Kanderi1, Mohammed AL-Otaibi2, Khalid AL-Abdulghani2 South Sabah Salem1 and Al-Rehab2 Clinic, Farwania Health Area, Kuwait. Code Number: gm09003 Aim: The objective of the study is to determine the availability of anti-hypertensive medications in primary care clinics in Kuwait, and the impact of such problem on the hypertensive patients, since hypertension is a major chronic illness with significant morbidity and mortality. Key words: Hypertension, medications, primary care. INTRODUCTION Hypertension is a polygenic disease defined as systolic blood pressure of 140 mmHg &/or diastolic blood pressure of 90 mmHg or greater (in three consecutive readings), in people who are not on anti-hypertensive medications (1,2). It is an important major risk factor for stroke, renal, and ischemic heart disease. Its control will significantly lower these diseases. It also causes almost half of the early deaths in individuals between 45 and 65 years of age worldwide (2). The control of hypertension is one of the biggest challenges facing public authorities and general practitioners .Clinical practice guidelines are considered worldwide as a corner in the process of delivering quality health care to the population. The development of these guidelines in primary care is one of the priorities in the strategic plan of the central department of primary health care for the coming years. These guidelines help the physicians to update their practical knowledge, particularly in establishing appropriate diagnosis of common and chronic illness, and in minimizing the range of discrepancy in management of those illnesses (3-8). The close working relationship between the world health organization (WHO) and the international society of hypertension (ISH) has existed for several decades and led to the production of a number of guidelines and statements. Since the publication of the 1999(WHO/ISH) guidelines for the management of hypertension, (WHO) determined in 2000 that in future the evidence base for all of its guidelines will be explicitly documented according to a defined methodology (9). Also the new guidelines issued by the Joint National Committee (JNC) on prevention, detection, evaluation and treatment of high blood pressure emphasize that aggressive blood pressure (BP) control is essential to reduce morbidity and mortality. Additionally, guidelines issued by the American Diabetes Association (ADA) emphasize the critical need for lowering blood pressure levels (10). Despite those guidelines, many patients’ blood pressure remains uncontrolled and in several instances, metabolic abnormalities and co-morbidities were apparently not considered while prescribing anti-hypertensive drugs (11,12). Unsatisfactory blood pressure (BP) control so often described in treated hypertensive populations is also explained by insufficient physician’s awareness of expert guidelines & their management according to a simple (BP) based approach rather than a more integrated approach based on global risk stratification. So a rational drug therapy approach is needed in treating hypertension to achieve better control rates (11). The primary goal of treatment of hypertension is to achieve maximum reduction in the total risk of cardiovascular morbidity and mortality. The goal of anti-hypertensive therapy should be able to restore blood pressure to levels defined as normal or optimal. Target (BP) levels are systolic <130 mmHg and diastolic <85 mmHg for young, middle aged and diabetic hypertensive and systolic <140 mmHg and diastolic <90 mmHg for elderly patients (2). The health care delivery system in Kuwait is divided into five health regions ; a number of primary care centers and one regional hospital serve each. Each primary care center serves a residential area. The majority of primary care centers are walk-in clinics where patients are treated for common medical problems and receive simple emergency care. Hypertensive patients often visit the primary care center for (BP) check-up under regular follow up as in hypertensive clinics or when they are out of treatment or symptomatic as in general practice clinics. There are few hypertensive clinics in Kuwait scattered mainly in family medicine centers where patients are followed up usually by a family physician and their (BP) is treated based on updated guidelines and annual investigation are requested . MATERIAL AND METHODS This is a descriptive study conducted during January 2006 focusing on studying and scrutinizing the availability of anti-hypertensive medications in primary care centers in Kuwait. A telephone call or face-to-face interview was conducted (between the clinicians and the pharmacists) among the pharmacist, of each primary care center about the availability of anti-hypertensive medications and the information was recorded in a standardized data collection form. Primary care centers are divided into two types: Family medical center (19 centers), which are staffed by certified physicians with structured training in a post-graduate primary care training programme, and a non-family medical centers (52 centers). All family and non-family centers were surveyed for this study. RESULTS A survey was conducted in all 71 primary care centers, registered under the Ministry of Health(MOH), to find out scrutinizethe availability of hypertension medications. All doses concentrations of atenolol & propranolol 10 mg were available in all centers. Propranolol 40 mg was available in only all Capital & Ahmadi health centers (HA), while none of the centers in Farwania or Jahra had it . Higher doses concentrations of propranolol (80, 160 mg) were available only in five centers of Capital area(HA). None of the centers had labetolol & carvidolol available while metoprolol was available in 12 centers situated within the capital HA only in Capital area. Diltiazem 60 mg was available in 33 centers; 8 in Hawalli, 4 in Capital, 12 in FarwaniaHA and in all Jahra clinics, while it was not available in Ahmadi centers. Higher doses concentrations of diltiazem was not available in any of the centers and low concentration of verapamil (40 mg) was available in 9 centers ; 8 in Capital area and one in Ahmadi. None of the potent Calcium channel blockers like felodipine, amlodipine or trimetazidine was available in any of the clinics surveyed. Nifedipine 10 mg has been withdrawn due to its drug-drug interaction with Beta-Blockers. Nifedipine 20 mg instead, was available in the centers. Captopril 12.5 mg was not available, while captopril 25 mg was available in almost all centers (70/71). Captopril 50 mg was available in 14/20 centers in Capital area, 7/9 centers in Jahra and in all clinics of Ahmadi, Hawalli and Farwania health area. Cilazapril 2.5 mg was available in 12 centers; six in Hawalli, one in both Capital and Ahmadi, two in both Jahra and Farwania areas. Other concentrations (1mg, 5mg) were not available. All concentrations of lisinopril were available in all Capital centers, almost all Ahmadi centers 12/13, 8/12 in Hawalli, 4/9 in Jahra and 9/17 in Farwania area. None of the centers had the lower dose of perindopril (2 mg). Higher concentration (4 mg) was found in 15/20 in Capital area, 4/13 in Ahmadi, 7/12 in Hawalli, 3/9 in Jahra and 8/17 in Farwania area. None of the other Angiotensin Converting Enzyme Inhibitors (ACEI) was available. In addition, all the centers lack any of the Angiotensin II receptor antagonists. Spironolactone was found in only 4 centers ; three of them in Hawalli and one in Ahmadi area. Only the lowest concentration of furosemide (40 mg) was found in all centers. Amiloride/hydrochlorthiazide was found in all Hawalli, Jahra, Farwania clinics, 18/20 of Capital and in 10/13 of Ahmadi centers. Chlorthalidone 25 mg was not available in any of the centers in Hawalli, Jahra and Farwania area, while it was found in 12/20 in Capital 3/12 in Ahmadi area. Chlorthalidone 50 mg, on the other, hand was available in 5/20 clinics in Capital area, 9/13 clinics in Ahmadi area, 8/9 clinics in Jahra area, 16/17 clinics in Farwania area and in all Hawalli health centers. Indapamide(SR) was found in almost all clinics in Capital area (19/20), 12/13 clinics in Ahmadi area, 9/12 clinics in Hawalli area, 13/17 clinics in Farwania area, and 6/9 clinics in Jahra area. From the last group surveyed, only methyldopa 250 mg was found in all centers. There was a statistically significant difference between family & non-family centers in terms of adequacy of some medications namely metoprolol (p<0.001) & all concentrations of lisinopril( 5mg, 10mg, 20 mg) (p<0.05). Indapamide(SR), on the other hand, although it was available in almost all family centers (18/19), it was also available in most of non-family centers (41/52). In fact the difference between family & non-family centers did not reach level of significance (p=0114). The differences are shown in Table 2. DISCUSSION This study shows that primary care centers in Kuwait lack essential, potent & effective medications for treating hypertension. This undoubtedly affects the quality of care. The fact we realized from this study that none of the centers had Angiotensin II receptor antagonists and potent Calcium channel blockers available, makes the management of hypertension very difficult for primary care physicians. The policy of (MOH) is to confine relatively expensive medications to secondary or tertiary care centers has created over-reliance of patients on these centers. The increasing costs are probably the main reason for the unavailability of these medications in primary care centers in Kuwait. Although using such expensive drugs increases the cost of hypertension medication, but it reduces the total health cost by corresponding reductions in other medical expenditure. The fact that family medicine centers had more medications available than the non-family centers reflects that the former are staffed by physicians with post graduate training in family medicine and are better provided with medications by the (MOH). These medications are requested only for Kuwaitis and prescribed only on registered files in the primary care clinics (e.g indapamide, lisinopril, perindopril, metoptolol and cilazapril). Currently, most of the family medicine centers are located in the Capital health region (10/19); hence, there is a plan to expand the family medicine network with more physicians graduated from the family medicine training programme. The absence of free essential hypertension medications is a barrier to adequate hypertension care in primary care centers, this result is in consistent with other studies (12,13). In conclusion, general access to these potent anti-hypertensive medications, coupled with proper training of primary care physicians in long-term management of hypertension will improve overall hypertension care in Kuwait similar to other studies conducted worldwide (11,14). Through the expansion of family medicine programme better hypertension management at the primary care level should be achieved. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09003t2.jpg] |
| |||||||||

{kind=link}