 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
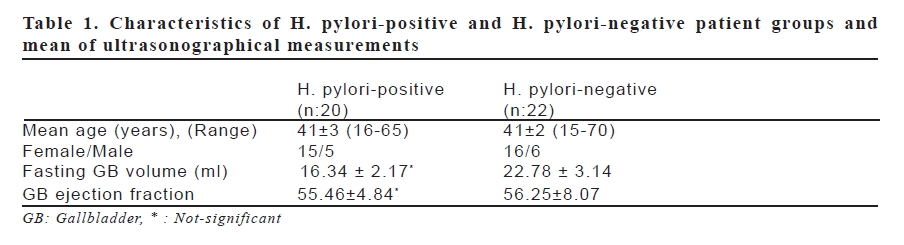
European Journal of General Medicine, Vol. 6, No. 1, 2009, pp. 15-19 Ultrasonographical Evaluation of Gallbladder Functions in Helicobacter Pylori-Positive and Negative Patients Mustafa Güçlü1, Tolga Yakar1, Ali Pourbagher2 Başkent University, Faculty of Medicine, Departments of Gastroenterology1 and Radiology2, Teaching and Medical Research Center, Adana, Turkiye Code Number: gm09004 Aim: Helicobacter pylori (H. pylori) infection is responsible for various pathologies in the stomach. It can be suggested that H. pylori may alter the effect of somatostatin on the gastrointestinal system, particularly having an effect on the D-cells in the antrum-located infections. Therefore, we planned to investigate the gallbladder functions ultrasonographically in H. pylori-positive and -negative patients. Key words: Helicobacter pylori, gallbladder functions, ultrasonography INTRODUCTION Helicobacter pylori (H. pylori) is the major etiological cause of chronic active gastritis, and plays an important role in gastric ulcer and duodenal ulcer. The H. pylori infection may change the gastric acid secretion. The gastric acid secretion decreases as a result of corpus gastritis caused by H. pylori infection, which is followed by the development of mucosal atrophy. The gastric acid secretion can be influenced by several factors like autonomous nervous system and gastrointestinal hormones. The major hormones having direct or indirect effect on the gastric acid secretion are gastrin and somatostatin (SST). SST is found in the epithelial endocrine D-cells in the mucosal layer of the gastrointestinal system (1). In the antrum, D-cells have apical membranes, and they are called open cells since they are associated with the lumen. In the corpus, D-cells are closed, and there is no connection between the mucosal surface and the lumen. In the antrum, the H. Pylori infection leads to a decrease of antral D-cells resulting in a decrease in the expression of SST, which inhibits the gastrin secretion (2,3). In the H. pylori-induced gastritis, there are severe anomalies in the secretion of gastrointestinal polipeptide hormones. Antral SST concentration and D-cell density decrease. SST is an inhibitory hormone of gastrointestinal system (GIS). Any decrease in the SST levels eliminates the pressure on the G-cells secreting gastrin, so the gastrin levels increase. Hypergastrinemia stimulates the acid expression from parietal cells, and leads to a damage in the duodenal bulber epithelium. Following the H. pylori eradication, SST concentration becomes normal, and similarly gastrin goes back to its normal levels (4-8). SST inhibits the secretion of cholecystokinin, gastrin, secretine and glukagon. It also inhibits the gastric and intestinal motility. It can be expected that H. pylori may have an effect on the gallbladder functions due to both its association with low levels of B12 and its decreasing effect on SST concentration by influencing the gastric D-cells. The relation between H. pylori and gallbladder functions are not well known yet. The present study aimed to evaluate the GB functions and contractility using ultrasonography (US) in H. pylori-positive and negative patients, and to assess the extent of the impairment. MATERIAL AND METHOD The study included 20 H. pylori-positive patients (mean age 41±3 years, 15 female and 5 male) and 22 H. pylori-negative patients (mean age 41±2 years, 16 female and 6 male) with a body mass index less than 30, diagnosed on the basis of the mucosal biopsies from antrum, corpus and fundus in upper gastrointestinal endoscopy performed for the evaluation of dyspepsia. All volunteers gave their written and informed consent to participate in the protocol, which had been approved by the Medical Ethics Committee of the Academic Medical Center of Baskent University. The patients with diabetes mellitus, hepatitis, biliary colic, any history of gastrointestinal surgery, chronic renal failure, chronic liver disease, diagnosis of autonomous neuropathy and systemic disease were excluded. Seventy-two hours before the study, all medications were discontinued. All cases underwent US in the morning after one-night fasting. During the US analysis, a Philips HDI 5000 equipment and a 3.25-5 MHz transducer were employed. During the fasting period, the morphology, wall thickness, lumen of the gallbladder were evaluated as well as the liver and the intra- and extra-hepatic biliary tracts. The cases with thickened biliary wall, stone, debris, polyp or cholesterol crystals in the lumen were excluded. After measuring the fasting width, length and depth of the gallbladder, all cases received orally a standard 100 gr chocolate (528 kcal; 58% carbohydrates, 35% fat, 4.5% protein). Postprandially at 120 and 180 minutes, the three dimensional measurements of the gallbladder were repeated, and from these measurements fasting volume, residual volume at 2 and 3 hours, maximum residual volume, maximum contraction period and ejection fraction were calculated. The lowest postprandial volume of the gallbladder was accepted as the maximum residual volume. Due to its elliptical appearance, the ellipsoid formula [V = π/6 (width x lenght x depth)] was used for calculating the volume. For the assessment of GB ejection fraction, formulation of fasting volume – maximum residual volume/fasting volume x 100 was used (9). Statistical analysis Student’s t test was used to determine and compare the differences between the two groups. The results were obtained as mean ± SD. Of the results, only the ones with a p value less than 0.05 were found significant. Data were analyzed using the SPSS for Windows (version 9.05; SPSS, Inc., Chicago, Illinois, USA). RESULTS The study included 20 H. pylori-positive patients (mean age 41±3 years, 15 female and 5 male) and 22 H. pylori-negative patients (mean age 41±2 years, 16 female and 6 male). In H. pylori-positive and -negative patients, the volumes were found as follows respectively; 16.34±2.17 ml and 22.78±3.14 ml for fasting GB volume; 8.24±1.65 ml and 12.22±1.93 ml for residual volume at postprandial 2 hours; 7.78±1.89 ml and 10.65±1.83 ml for residual volume at postprandial 3 hours; 8.55±1.47 ml and 12.131±1.98 ml for residual volume after maximum contraction; and 55.46%±4.84 and 56.25%±8.07 for GB ejection fraction (Table 1). The volumes of fasting GB and postprandial 2 and 3 hours were slightly lower in H. pylori- positive patient group compared to H. pylori-negative patient group. However, for all parameters compared between the two groups, no statistically significant difference was found. DISCUSSION The patients infected with H. pylori had a decrease in the antral SST concentrations as well as in the SST levels of gastric fluid (3). The H. pylori infection changes the concentration of regulatory peptides such as SST, gastrin and cholecystokinin in the gastric mucosa (10). SST is the major inhibitory hormone of GIS. The role of GB dismotility and GB hypomotility, particularly on the formation of gallstone is well known. Although many GIS hormones have an influence on the GB functions, among all the most important ones are mainly cholecystokinin (CCK), secretine, gastrin and glucagon. SST is the main inhibitory peptide of GIS. A study compared the serum gastrin and SST concentrations in 37 H. Pylori-positive and 29 H. Pylori-negative cases. The serum gastrin level was higher in H. pylori-positive patients compared to H. pylori-negative cases, however in H. pylori-positive patients particularly with duodenal ulcer, the serum SST levels were found significantly lower than the levels in patients without duodenal ulcer (1,11). This study shows that H. pylori infection suppresses SST secretion (1). There is a possibility of abnormal functioning in the organs, which were influenced by the autonomous nervous system and CKK hormones. Therefore, some abnormalities can be expected in other organs influenced by the same systems as well (12,13). The autonomous nervous system and CCK play a major role in the GB discharge and normal functioning (14). The regulation of GB functions is under the control of autonomous nervous system and hormones (15,16). The cholinergic system helps in the continuity of GB tonus between the eating and digestion periods as well as GB contractions occurring after the meals (15). GB functions are impaired in diabetes mellitus patients with autonomous neuropathy and in postvagotomic subjects (17,18). In a study it was shown that abnormal vagal functions have an effect on the gastrointestinal tract, and it is likely to see abnormalities of GB functions in those patients (19). It has been demonstrated that the discharging functions are damaged in subjects who developed diabetes-induced autonomous neuropathy or underwent vagotomy (17,18). As it is well known, the regulation of GB functions are under the control of neuroendocrine hormones such as cholinergic system and CCK. While the autonomous nervous system, i.e. the cholinergic system helps the contraction of the gallbladder during eating and digestion, it also provides maintenance of the biliary tonus during the period between the meals (17,18). Usually GB discharge is under both neural and hormonal control. For biliary flow, the GB contraction is accompanied by the relaxation of Oddi sphincter, and GB discharge can be impaired by any abnormality in any of them (15). In order to mention any GB dysfunctioning, the ejection fraction must be decreased 40% according to the Rome criteria 1998 (20). In the present study, no significant difference was found between H. Pylori-positive and –negative patients in the GB ejection fractions, and values were within the normal range. These results demonstrate that there is no difference between H. Pylori-positive and negative patients in terms of the GB functions. However, in the present study it was found that the H. pylori infection didn’t affect the GB functions. So our findings indirectly show that the GB functions are damaged neither by the systemic effect of SST nor the autonomous neuropathy possibly due to lack of vitamin B12 in the H. pylori infection. H. pylori DNA is common in the gallbladder of patients with gallstone, however it may not play a remarkable role in the formation of gallstones alone. In recent studies about the effect of H. pylori on the gallstones and gallbladder, H. pylori DNA was detected in the GB tissue, formation of gallstone and biliary content of H. pylori (21). Therefore, Helicobacter is thought to be associated with cholecystitis and cholecystolithiasis (21). In recent years, it has been suggested that Helicobacter species can be colonized in the biliary system, it can play a role in the pathogenesis of hepatobiliary cancer and it can change the kinetics of biliary system cells (22). CCK also plays a major role in the postprandial motor activity just like it does in the GB functions. In patients with duodenal ulcer, it is likely to occur some abnormalities in the gastric motor activity. In the present study, which evaluated the GB functions between H. pylori-positive and negative patients, no relation was found between fasting GB volume, GB volumes at 120 and 180 minutes and GB ejection fractions. However, a slight reduction was observed in the GB functions of H. pylori-positive patients. To our knowledge, the only study, which investigated H. pylori and GB functions was carried out by Marzio L et al and they have found no significant difference between H. pylori-positive and negative patients given oral 340 kcal in dyspeptic patients (23). In our study, GB functions with higher calories (528 kcal) and longer periods (180 minutes) were evaluated, however no significant difference was found between GB functions and GB ejection fractions in H. pylori-positive and -negative patients, which is also supporting the study by Marzio L et al. In conclusion, our study suggest that there is no relation between H. pylori status and GB functions evaluated the US. To obtain more data on the effects of H. pylori on GB functions further studies including case-controls are needed. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09004t1.jpg] |
| |||||||||

{kind=link}