 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
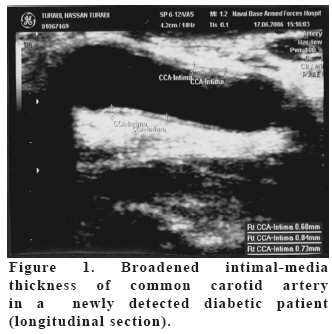
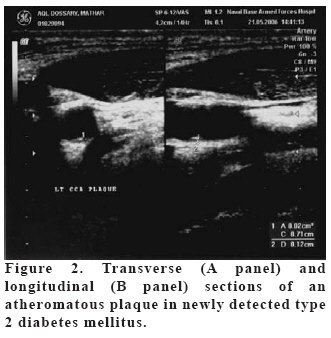
European Journal of General Medicine, Vol. 6, No. 1, 2009, pp. 28-37 Generalized Vascular Damage Including Glomerular Dysfunction in Newly-Detected Type 2 Diabetic Patients Hamdy Abo-Zenah1, Moharram M2, Imran A3, Quazalbash S3, Al-Benayan A4, Sabry A5 King Abdulaziz Naval Base-Armed Forces Hospital, Departments of Internal Medicine1, Radiology2, Ophthalmology3, and Medical Administration4, Jubail, Saudi Arabia In Collaboration with 5Prince Salman Nephrology Center, Saudi Arabia Code Number: gm09007 Aim: Diabetes mellitus (DM) is considered a vascular disease, we intended to determine prevalence and nature of generalized and glomerular vascular abnormalities the moment it is diagnosed (ND-DM) in a cohort of patients with Arabic descent. Over 9 months, 216 out of 1208 asymptomatic Saudies were referred by the Primary Care Physicians on having risk factors for future development of DM for DM screening. Key words: Intimal-medial thickness, albuminuria, retinopathy, diabetes, Saudi Arabia INTRODUCTION Diabetes Mellitus (DM) is a highly prevalent chronic complex metabolic disease. The prevalence of diagnosed and undiagnosed DM in people aged 20 years and older is enormously increased world-wide. In USA, it rose by about 30% from 4.9% in 1996 to 6.9% in 1999 (1) with 90-95 % of them having type 2 disease (T2DM) (2). In United Kingdom (UK), more than three percent of population has diabetes, and about the same number again can be found on screening studies (3). A much higher prevalence (23%) has even been reported in the gulf region (4). The exact prevalence might be higher as approximately one-third of population with diabetes may be undiagnosed (5). Type 2 DM is a major contributor of morbidity and increased mortality. Micro-vascular complications like diabetic nephropathy (DN) and diabetic retinopathy (DR) are major causes of morbidity in diabetics. Diabetic nephropathy is the single leading cause of end-stage renal disease (ESRD) and more than 50% of US patients receiving dialysis treatment have T2DM (6). Persistent microalbuminuria (µA) (30–299 mg/day) has been shown to be the earliest stage of DN in type 1- and a marker for development of nephropathy in T2DM. Albumin permselectivity and therefore (albumin excretion rate) AER at the glomerular level is first determined by the glomerular basement membrane (GBM) (7) with podocyte-slit diaphragm structure operates more efficiently as a second finer filter (8). Likewise, diabetic retinopathy (DR) is a highly specific vascular complication of both T1 & T2DM and was estimated to be the most frequent cause of new cases of blindness among adults aged 20–74 years (9). Also, diabetics are 2-4 times more likely to have cardiovascular disease (CVD) than non-diabetics leading to awareness of DM as a heart disease equivalent (10) because of its strong association, especially type 2, with increased risk of atherosclerosis (11, 12). Precisely, ischaemic heart disease, other heart diseases, and cerebro-vascular diseases account for 40, 15, and 10% of all deaths in diabetic population, respectively (13). Unfortunately, in women, diabetes may eliminate the CV protective estrogenic effect (14). So far, there is no information on the exact prevalence and nature of generalized and/or glomerular early vascular damage in ND-T2DM classified according to the new American Diabetes Association criteria among patients of Arab origin. We therefore screened for common carotid artery- (CCA) intimal-media thickness (IMT) and/or plaques as well as nephropathy and retinopathy in them, in comparison to healthy subjects. In addition, we investigated the relationship between various risk factors and markers of vasculopathy in study population. This is a prospective, cross-sectional, controlled estimation of vascular abnormalities prevalence in ND-T2DM and their relation to CVD risk factors. For that we measured CCA-IMT as a marker of early macro-vascular disease as well as retinopathy and glomerulopathy as markers of micro-vascular disease in comparison with age-matched healthy individuals who have normal glucose tolerance. MATERIAL AND METHODS Subjects In accordance with our institutional guidelines, the protocol was approved by Medical Research and Ethics Committee. All patients were aware of the investigational nature of this study and its aim. Asymptomatic middle-aged (35–60 years) Saudi adult individuals (n=216, 171 males & 45 females out of 1208) who attended the Primary Care Department at Jubail Military Hospital, Saudi Arabia for 9 months (September 2005 to May 2006) were consecutively referred on having any of the risk factors reported by Engelgau and associates (2000) for future development of diabetes (5). Exclusion criteria included non-Saudi residents, known diabetes & hypertension, and medication that could affect glucose tolerance such as thiazide diuretics, β-blockers, or corticosteroids. Eighteen male subjects among the hospital staff, matched for age, were enrolled as control group. Exclusion criteria for healthy controls were cardiovascular disease (CVD), treatment with CV drugs and abnormal glucose homeostasis. Included subjects were candidates for oral glucose tolerance testing (OGTT) using 75 gm anhydrous glucose dissolved in water. The test was performed as described by World Health Organization (WHO) (15). Plasma glucose was measured by hexokinase method (interassay coefficient of variation (CV)=1.5%). Newly-diagnosed Diabetes mellitus (ND-DM) was present in those who have not reported a previously diagnosed diabetes and according to the American Diabetes Association (ADA) new criteria that included a 2-h Post-Glucose level of ≥ 11.1 mmol/L during an OGTT or a fasting (>8h) plasma glucose of ≥ 6.1 mmol/L (16) . Once newly-diagnosed as having T2DM (n=54, 41 males & 13 females), thorough clinical examination was done including fundus examination by knowledgeable ophthalmologists (Dr. Imran A and Dr. Quazalbash S) after pupillary dilatation. Anthropometric determinations were made following the standard protocol described by Lohman and colleagues (1982) (17) for body mass index (BMI) that was calculated as body weight (kilograms) divided by height squared (meters). The waist circumference was determined with a plastic measuring tape at the midpoint between lower rib margin and iliac crest, and hip circumference, at the level of trochanter. The ratio between them provided waist-to-hip ratio (WHR). Hypertension was defined as a persistent elevation of blood pressure greater than 140/90 mm Hg or the use of anti-hypertensive medications based on Guidelines Sub-Committee of the 1999 World Health Organization-International Society of Hypertension Guidelines for the Management of Hypertension (18). Methods At the time of vital signs measurements, a freshly-voided, clean-catch, mid-stream urine (MSU) sample was taken for albuminuria evaluation using Micral-Test strips (Roche Diagnostics, Meylan, France). The Micral-Test II strip permits an immediate and reliable semi-quantitative determination of low albumin concentrations in urine samples with an almost user-independent color interpretation (19) and a sensitivity of up to 94% and specificity between 83-93% (20). Moreover, it is easy to handle with a short reaction time and a stable colour reaction that is easy to read (21). Additional laboratory investigations included serum creatinine (sCr), estimated glomerular filtration rate (e-GFR), fasting total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), CRP, and glycosylated hemoglobin A1C (A1C). We measured A1C using Bio-Rad Variant Hemoglobin A1C Testing System, US Bio-Rad Laboratories Inc, Hercules, CA, USA. The test type applied was Ion Exchange High Performance Liquid Chromatography (22) with the use of Variant A1C reorder pack (Cat. No. 270-0003). The normal range for the used reagent is 4.1-6.5%. Fasting TC, TG, HDL-C and CRP were evaluated using the standard laboratory techniques and the eGFR was calculated based on the 4 variables MDRD formula: eGFR(ml/min/1.73 m2)=186 x {(sCr (mg/dL)/88.4)-1.154} x age (years) -0.203 x 0.742 if Female x 1.21 if Black. Common carotid artery (CCA) examination High-resolution B-mode ultrasound examination of common carotid artery (CCA) was performed with Voluson 730 pro (GE Medical System Ultrasound, Kretztechnik, Gmb H & Co OHG, Austria) as a non-invasive tool with a 5-10MHz multifrequency linear transducer (23) to measured intimal-medial thickness (IMT) bilaterally. The software program of the scanner is provided with the option of quantitative measurements of IMT in a fraction of 0.01mm. Briefly, we measured IMT of far wall in plaque-free segments as originally described by Pignoli and colleagues (1986) (24) on the same day of blood collection. Sonography and readings were carried out by trained radiologist (Moharram M) who was unaware of the corresponding laboratory values. To avoid variability during the cardiac cycle, the images were frozen in the end-diastolic phase. With each scan of CCA, 1–2 cm proximal to the bulb, IMT was measured twice bilaterally and the mean of these values represented IMTmean of each subject. Further, each carotid wall and segment was examined independently from continuous angles to identify the thickest intimal-medial site (IMTmax). For this study, IMTmean as well as IMTmax were calculated and as they were significantly correlated (r=0.54, P<0.001), the analysis was performed with only IMTmax. For carotid plaque assessment, both near and far walls of all CCA segments were scanned longitudinally and transversally and a plaque was present when a localized echo structure encroaching into the vessel lumen and protruded more than 50% of adjacent parts of intimal- media layer was detected. The measurements of plaque thickness were made using computerized system at the site of maximal encroachment perpendicularly to vessel wall by measuring the distance between media-adventitia interface and lesion surface facing the lumen as previously prescribed (25). Statistical analysis Data for all considered variables had a normal distribution and were expressed as mean ± SD unless stated otherwise. Fisher’s exact test was used to compare the prevalence of non-parametric variables while differences between variables were analyzed by paired Student’s t test or Mann- Whitney test as deemed appropriate. The relation between measurements was assessed by Pearson’s correlation for parametric and Spearman’s correlation for binary variables. A p of < 0.05 was considered statistically significant. All analysis was performed using the Statistical Package for Social Science (SPSS, Chicago) version 10.0 for windows. RESULTS We screened, through the Primary Care Department, 1208 Saudi adult individuals who fulfilled the inclusion criteria of this study over nine months (September 2005 to May 2006). The primary care physicians referred 216 (171 males and 45 females) subjects out of the 1208 representing about 18% of the screened sample who were at risk for future development of diabetes mellitus (DM). After OGTT, 54 patients (41 males and 13 females) were found to be diabetics according to the American Diabetes Association (ADA) new criteria with a mean age of (39±4.8 years) and they represented 4.47% of the surveyed sample. The newly-diagnosed diabetics (ND-DM) had significant (p=0.01) preclinical atherosclerosis in the form of increased Intimal-Media thickness (IMT) and/or atheromatous plaques in CCA (35 out of 54) compared to controls (5 out of 18). The increased IMT was observed in 24 ND-DM compared to only 4 controls as seen in Figure 1, while atheromatous plaques were noted in 11 patients (Figure 2) versus only one healthy subject. The ND-DM patients had significantly broader IMT compared to controls, as seen in table 1, and they were heavier (higher BMI), with more visceral obesity (WHR), hyperlipidaemia (except HDL-C), pathologic albuminuria and higher blood pressure (BP) although they were comparable in age, eGFR and CRP levels. The correlates of IMT are age (r=0.389, p=0.004), male gender (r=0.342, p=0.011), WHR (r=0.426, p=0.001), TC (r=0.29, p=0.041) and TG (r=0.269, p=0.049). There was no association between IMT and BMI, A1C, CRP or HDL-C. Table 1. Characteristics of both newly-diagnosed diabetics and their controls.
Abbreviations: IMTmax=maximum intimal-media thickness, BMI=body mass index, WHR=waist to hip ratio, SBP=systolic blood pressure, DBP=diastolic blood pressure, A1C=glycosylated hemoglobin A1C, eGFR=estimated glomerular filtration rate, TC=total cholesterol, TG=triglycerides, HDL-C=high-density lipoprotein cholesterol, and CRP=C-reactive protein. Within the newly-detected diabetics, the differences between those with increased IMT and/or plaques (n=35) and those (n=19) with IMT measurements within the controls’ values (0.67±0.05 mm) are displayed in table 2. They were older with heavier body weights, more abdominal obesity, TC, TG, and urinary albumin excretion (UAE) rates. However, both subgroups showed non-significant (NS) differences in their BP, glucose homeostasis, CRP, and HDL-C values. Table 2. Comparison between patients with increased- and those with normal-IMT within the ND-DM study cohort
Abbreviations: ND-DM= newly-detected diabetes mellitus, and the rest are as Table 1 Glomerular dysfunction and diabetic nephropathy (DN) as defined by urinary albumin excretion (UAE) of ≥30 mg/day was present in 17 out of the studied 54 ND-DM patients and its prevalence was statistically significant (Chi-squared, p=0.014). Among the ND-DM cohort of patients, those with increased UAE (DN) have more preclinical atherosclerosis (IMT=0.96±0.1 vs 0.77±0.1, p=0.0001), lower eGFR (86.4±12 vs 104.1±13, p=0.0001), older age (40.9±5 vs 37.9±4, p=0.028), more abdominal obesity (WHR=0.98±0.1 vs 0.91±0.13, p=0.037), higher TC (5.4±0.7 vs 4.9±0.9, p=0.049) and TG (2.7±0.4 vs 2.02±0.4, p=0.012), with worse glycemic control (A1C=8.1±1.6 vs 7.3±1.5, p=0.048). However, they both have comparable BP, BMI, and HDL-C levels. Of note, the eGFR was within the normal range in all but one patient who had stage 3 (eGFR=41 ml/min) chronic kidney disease (CKD) according to the NKF/KDOQI guidelines. Also, we have detected a significant prevalence (n=19) of diabetic retinopathy (DR), another marker of vascular abnormalities, in our ND-DM patients (chi-squared, p=0.047). Most of patients (n=14) with DR showed background type with few (n=5) displayed mild-moderate proliferative DR. None suffered from severe proliferative DR, blindness or were partially-sighted on their referral to ophthalmology assessment. Interestingly, both type of microvascular changes, DN and DR, were significantly correlated with each other (r=0.841, p=0.0001). Further, with the application of non-parametric Spearman’s correlation, macrovascular abnormalities in the form of increased IMT correlated significantly with the prevalence of DN (r=0.38, p=0.005) as well as with DR (r=0.35, p=0.009). DISCUSSION We observed in this screening a 4.47% prevalence of undiagnosed diabetes mellitus (DM) among our study population. This is in line with the prevalence detected by National Health and Nutrition Examination Survey (NHANES III) in USA (26) and by Cardiovascular Health Study (CHS) (27) but was much lesser than that (27%) known to be present in the Saudi community (4) because of periodic screening performed by Primary Care Department on one hand and because the Check-up on patient’s request is accepted according to our hospital Policy and Procedure on the other hand. Of note, an even higher prevalence of ND-DM (39%) than that noted in the general Saudi population was reported by the insulin resistance atherosclerosis study (IRAS) in another ethnic group, the African-Americans (28). We detected generalized vascular damage, as inferred from increased intimal-media thickness (IMT), in a substantial proportion of our Saudi patients with newly-detected T2 DM (ND-DM) although its degree was much lesser than that noticed in other studies. Such studies considered patients with an IMT <1 mm as normal, IMT between 1 and 1.3 mm as having wall thickening, and those with an IMT >1.3 mm to have plaque (29, 30). Our study cohort has different genetic backgrounds with a much lower normal measurement of IMT as noted in healthy control individuals. However, the remarkable prevalence of such preclinical atherosclerosis detected in this investigation was in line with a relatively recent study by Hunt and colleagues (2003) (31). The presence of atherosclerosis in the prediabetic state is not unexpected as the clock for macrovascular disease could start ticking before the onset of clinical diabetes (32) even if hyperglycaemia is still asymptomatic (33). The presence of the observed ultrasound-assessed atherosclerosis along with increased cardiovascular risk by the time of DM detection was in concordance with the report of a previous study (34) and could be explained by the Common Soil Theory hypothesized initially proposed by Jarrett and Shiply (1988) (35) and confirmed later by Stern MP (1996) (36). The factors we observed to be associated with high CCA-IMT were age, male gender, WHR, TC and TG, and not BMI, A1C, CRP, or HDL-C. Of the lipid parameters, TC and TG but not HDL-C was noted as one of the correlates of pre-clinical ultrasound-assessed atherosclerosis. Our observation is in sharp contrast to the findings of Sigurdardottir and colleagues in 2004 (37). The simple explanation is that the metabolic syndrome underlying T2DM in the Arabian Peninsula (38, 39, 40) may differs in its metabolic disturbances patterns from that described in other populations (41, 42, 43) including South Asians (44) being associated with raised plasma cholesterol and triglyceride rather than with low HDL-C levels. The significance of aging was already highlighted by other investigators (45, 46) and the WHR is believed to be an important parameter for cardiovascular risk assessment that should be determined on a routine basis (47). However, failure of CRP to correlate in this study with IMT is in harmony with the notion that it is not per se a major independent cause of early arteriosclerosis and that its elevations may mediate the effect of certain conventional risk factors on promoting widespread vascular damage atherogenesis (48). Further, the CRP we measured in this investigation is not the high-sensitivity type (49). We have shown in this screening that glomerular dysfunction in the form of increased microalbuminuria (µA) is there by the time of diagnosing DM in a considerable percentage of patients. For type 2 disease, persistent µA (30–299 mg/24 h) has been shown to be a marker for development of glomerular damage and diabetic nephropathy (DN) and it might be present even for years before clinical presentation as stated by Mogensen and associates (2003) (50). We have no accurate data neither regarding the course nor the incidence of diabetic kidney disease in the Saudi population. What is known in one unit is that the prevalence of DM among patients admitted to dialysis in 1999 was 40.5% (51) and that the vast majority (96%) of Saudi diabetics entering dialysis are of Type 2 (52). The presence of increased urinary albumin excretion rate (UAE) is alarming but not pessimistic. The investigators of the United Kingdom Prospective Diabetes Study (UKPDS) reported an annual rate of 2–3% per year for the transition between successive stages of increased UAE to end-stage renal disease (ESRD) suggesting that many individuals will not necessarily progress to worse kidney outcomes, even after developing microalbuminuria (53). Such finding was further recently supported by the observation, over a median of 15 years from diagnosis of type 2 diabetes, of nearly 40% of UKPDS patients developed albuminuria and nearly 30% developed renal impairment and both are not linked inexorably in type 2 diabetes (54). Risk factors of vascular dysfunction such as the ones reported in this study including abdominal obesity, hyperglycaemia and hyperlipidaemia might explain the detected glomerulopathy as concluded by Fox and co-workers (2005) (55). However, the prevalence of µA and DN in our ND-DM patients was much lower than the one-third reported by Kramer and co-workers (2005) (56). The diverging result may be the effect of variable ethnicity, and their inclusion of both long-standing asymptomatic and recent-onset newly-diagnosed DM which was not the case in this survey. The majority of our Saudi population with ND-DM (65%) had increased IMT while a much lower proportion of them (31%) displayed evidence of glomerulopathy. This is in concordance with the notion that microalbuminuria and DN do develop in only from 20–40% of the patients as concluded by the group of Faronato (1997) (57) while cardiovascular complications are observed in a much higher percentage of them, even without microalbuminuria (58, 32). Also, our findings support the definition adopted by the European Guidelines for Hypertension Diagnosis and Treatment that microalbuminuria is a risk factor for cardiovascular events besides being a marker of target tissue damage at the kidney level (59). It is well-known that albuminuria reflects a widespread vascular damage due to a generalized vascular dysfunction at endothelial and/or glomerular levels (60). The presence of diabetic retinopathy (DR) we showed in our newly-detected diabetics by the time of DM detection is in concordance with a similar finding in UK (61) though we failed to report marked loss of vision in any of our patients at screening as observed in another study (62). This DR was observed in considerable prevalence and this was more or less equivalent to what has been found among another Asian population (26.1%) (63). The presence of DR is alarming as it was estimated to be the most frequent cause of new cases of blindness among adults aged 20–74 years. Among the younger subjects (20-59 years), DR is still the most prevailing cause of blindness in Denmark (64) and in the over 65’s figures it has been more than doubled since 1990-1991 (65). Further, the observation of DR by the time of awareness of DM was concluded to have a predictive value for future development of DN in the form of pathologic albuminuria in type 2 British (54) as well as Saudi Diabetics (66). The early detection of vascular complications in this survey is supported by the fact that diabetes was considered by some authorities to be a vascular disease (67). This was reported for generalized vasculopathy including both macrovascular disease such as coronary artery disease (CAD) which was a frequent finding in prediabetic individuals and in T2DM patients at the moment their disease is diagnosed (32) as well as for microvascular alterations such as glomerulopathy and retinopathy that may precede the diagnosis of diabetes (68). Of DM duration, a threshold effect for atherosclerosis (28) and a graded effect for microvascular complications seem to operate (69). Such early detection of vascular complications in newly-diagnosed diabetes might be of great help. This is true at the level of macrovascular disease as most of mortalities among diabetics are due to CAD (70). Likewise, an effective screening and early treatment programme could reduce diabetes morbidity by increasing the chances for detection and subsequent institution of protective measures that may lower the burden of both ESRD and cardiovascular morbidity and mortality, as stated by Manjunath and colleagues (2003) (71) and as well for reducing the risk of blindness by more than half (72) using standard laser therapy (73). Limitations; our study population was limited to Saudi individuals and more so was not population-based and this might undermine generalization. Also, Serum creatinine was estimated once in this modest-sized cross-sectional investigation. Lastly, we have just recently introduced in our hospital the high-sensitivity CRP. In conclusion, the newly-detected diabetics already had more vascular changes in general and glomerular one in particular than age-matched, normal glucose-tolerant subjects. They exhibit a higher degree of early atherosclerosis as well as diabetic nephropathy and retinopathy with clustering of cardiovascular risk factors in particular abdominal obesity and dyslipidaemia in the early phases of diabetes. Acknowledgment The authors are grateful to the appreciated effort spent by the Primary Care Physicians, King Abdulaziz Naval-Base, Armed Forces Hospital, Saudi Arabia in the initial screening and subsequent referral of this study cohort. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09007f2.jpg] [gm09007f1.jpg] |
| |||||||||

{kind=link}
{kind=link}