 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
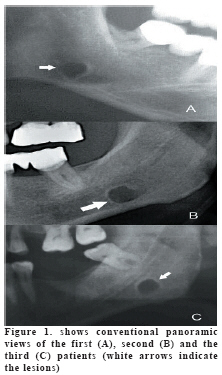
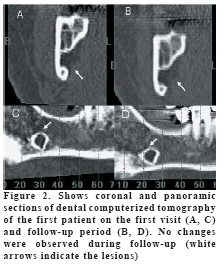
European Journal of General Medicine, Vol. 6, No. 1, 2009, pp. 42-45 Diagnosis of Stafne’s Bone Cavity With Dental Computerized Tomography Doğan Dolanmaz1, Osman A. Etöz1, A. Alper Pampu1, Erdem Kılıç1, Yıldıray Şişman2 Selcuk1, Erciyes2 and Karadeniz Technique3 University, Faculty of Dentistry, Departments of Oral and Maxillofacial Surgery1,2,3 and Erciyes University, Faculty of Dentistry Oral Diagnosis and Radiology4 , Konya1, Kayseri2,3 and Trabzon3, Turkey. Code Number: gm09009 Stafne’s bone cavity (SBC) is asymptomatic radiolucent lesion of the lower jaw and generally seen incidentally during routine radiographic examinations. Diagnosis of this lesion is essential because of its similarity with other odontogenic pathologies. We present three cases of SBC which was firstly diagnosed with plain radiographs that were confirmed with dental computerized tomography. Asymptomatic radiolucent lesions of the mandible should be confirmed with advanced imaging techniques in order to avoid unnecessary surgery. Key words: Stafne’s bone cavity, dental computerized tomography INTRODUCTION Stafne’s bone cavity (SBC) was first described by Stafne in 1942. He reported 35 asymptomatic unilateral radiolucent cavities in the posterior region of the mandible. Lesions were located between mandibular angle and the third molar, below the inferior dental canal and above the mandibular basis (1). Many different terms have been introduced like static bone cyst, lingual mandibular bone defect, idiopathic bone cavity and lingual mandibular bone depression in order to define the lesion (2,3). However the term SBC corresponds to the posterior lingual type which is the most frequent variant of the lesion (4). Anterior lingual type of the lesion is seen 7 times less frequent and usually located between the lower incisor and the premolar areas (5). SBC is generally encountered incidentally on routine plain radiographs and differential diagnosis includes odontogenic cyst and tumor like lesions (6). The aim of this paper was to present three case reports of SBC which were diagnosed with dental computerized tomography. CASE 1 A 55 year-old male patient was referred to our clinic by his dentist with an asymptomatic radiolucent area which was detected incidentally during routine dental examination. Panoramic radiograph revealed a unilateral well-defined unilocular radiolucent lesion on the right third molar region below the inferior alveolar canal slightly above the basis mandible (Figure 1A). Dental computerized tomography (DCT) scanning was performed to attain definitive diagnosis. Buccolingual images which revealed a lingual defect at the third molar tooth level, confirmed the final diagnosis of SBC (Figure 2A, C). Patient was informed about the lesion and scheduled for follow-up course. Approximately 4 months after the first appointment, no dimensional alterations were detected in DCT follow-up (Figure 2B, D). CASE 2 A 58 year-old male patient applied to the department of prosthetic dentistry for dental management. The panoramic view of the patient exhibited a well-defined radiolucent area at the level of third molar on the left mandible which was located below the inferior alveolar canal (Figure 1B). The second left mandibular molar tooth was asymptomatic. The patient was informed about possible odontogenic pathologies and surgical interventions and referred to our clinic. We performed a DCT scan in order to achieve the definitive diagnosis of the lesion. DCT showed a lingual bone depression at the level of the left mandibular third molar region which revealed characteristic features of SBC (Figure 1A, B). Information was given about the lesion and the patient is still in the follow-up course. CASE 3 A 46 year-old male patient who were suffering from pain from the right side of his face submitted to our clinic. A well-defined radiolucent area in the left posterior region of the mandible below the inferior dental canal at the level of the third molar was seen on the panoramic view of the patient (Figure 1C). DCT scan revealed that the lesion exhibits typical features of SBC (Figure 3C, D). The patient was notified about the lesion and scheduled for follow-up. DISCUSSION SBC is frequently located in the posterior lingual region of the mandible. This common variant of SBC has a quite rare occurrence (0.1% - 0.48%) when diagnosed radiographically. However some cadaver studies revealed that the incidence of the lesion may increase up to 6.06% (2,3,7). This difference may be due to asymptomatic characteristic of the lesion. SBC usually occurs in 5. and 6. decades of life and more common among males. Philipsen et al. in their comprehensive study, showed a 6:1 male/female ratio for SBC (2). Gomez et al. also reported 11 cases of SBC in whom 8 were men (4). The patients in the present report were at the 5. decades of their lives and all of them were males. Despite numerous theories regarding to the etiology of SBC, Stafne proposed the hypothesis that the lingual cavity was occupied by cartilaginous tissue due to bone deposition deficiency (1). On the other hand, the most widely accepted concept is pressure of the glandular tissue on the lingual cortex of the mandible (8). According to this concept submandibular salivary gland is responsible for the posterior lingual variant of the lesion while sublingual gland causes the anterior lingual variant (9). Hence, many investigators have found glandular tissue within the defect (4). Additionally Shibata et al. reported healing of the cavity after removal of the glandular tissue inside the lesion (10). Rare case reports have also been published regarding to muscular, lymphatic or vascular tissues related with the cavity (11,12). SBC is generally encountered incidentally on routine plain radiographs and differential diagnosis includes odontogenic cyst and tumor like lesions (12). However conventional radiographs may be inadequate for recognition of the lesion and needed to be supported with additional diagnostic techniques. DCT, Computerized tomography (CT), magnetic resonance imaging (MRI) and sialography techniques have been used to achieve final diagnosis of SBC. Gomez et al. proposed that CT is complementary diagnostic procedure for SBC and other cystic lesions could be distinguished with this method (4). Segev et al. declared that detection of SBC with CT is easier than MRI but they also mentioned that MRI should be considered in order to identify the content of the cavity (6). MRI is suggested for definitive diagnosis of SBC and reported to have less radiation exposure than CT (13). For CT images, larger cavities of SBC may be perceived smaller than they were and contents of cavities were uncertain (13). MRI has also some disadvantages like cost, discomfort to patient and possible image distortion. Sialography is also a diagnostic technique to determine whether glandular tissue exists in the cavity. However this procedure is invasive and uncomfortable for patient (14). DCT procedure is reported as a noninvasive easy method (15). It allows definitive diagnosis and can be used in follow-up period. Thus, radiographic follow-up is recommended management for SBC instead of surgery (16). In summary, the present report is probably the first in which asymptomatic bony defects were identified via DCT images. Lingual bone depression is evident in DCT which is the distinctive aspect of SBC. Thus DCT scans provide detailed information about definitive diagnosis of SBC. Panoramic radiographs may ensure somewhat initial opinion regarding to the diagnosis of SBC for experienced practitioners and might be used for follow-up of SBC cases. Clinician should be aware of suspicious radiolucent lesions of the mandible and should apply multiple imaging modalities in order to avoid unnecessary surgery. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09009f3.jpg] [gm09009f1.jpg] [gm09009f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}