 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
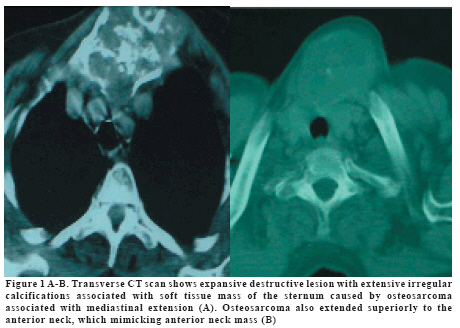
European Journal of General Medicine, Vol. 6, No. 1, 2009, pp. 46-48 Computerized Tomography Findings of a Sternal Osteosarcoma Güner Sönmez1, Ersin Öztürk1, Hakan Mutlu1, A. Rauf Görür2, Ali Kutlu3, Mahir Mahiroğulları4, Onur Sıldıroğlu1 , Çinar Başekim1,Eşref Kızılkaya1 GATA Haydarpasa Military Hospital, Departments of Radiology1, Thorax Surgery2, Chest Diseases3 and Orthopaedic Surgery4, İstanbul, Turkiye Code Number: gm09010 A 58-year-old female patient presented with chest pain and swelling in her neck. Computerized tomography showed an expansile mass containing lytic-sclerotic areas that caused destructions in the manibrium sterni and extended as far as to the thyroid gland at the lower cervical region and the upper mediastinum. Since osteosarcoma of the sternum is a extremely rare entity, we have thought to explain radiologic approach based on our experience. Key words: Osteosarcoma, computerized tomography, sternum INTRODUCTION Malignant bone tumors of the chest wall and sternum are more rare because most bone tumors occur in the long bones or joints.Osteosarcoma (OS) is a malignant bone tumor that occurs in the second or third decade of life. The men/women ratio is about 3:2 and half of the tumors occur near the knee. The most commonly occurring malignant tumor in sternum is chondrosarcoma and occurrence of osteosarcoma in sternum is extremely rare (1,2). For the radiological examination x-ray, computerized tomography (CT) scanning and magnetic resonance imaging (MRI) can be used. Among these the CT scanning is a valuable diagnostic method as it shows the peripheral soft tissue component and the intrathoracic spread of the tumor. In this report, we present the CT findings of a case with sternal OS. CASE A 58-year-old female patient was admitted with chest pain, swelling in her neck and occasional dyspnea complaints, which started one year ago and became intensified in the last three weeks. In the physical examination a lesion which was 10x8 cm in size, quite hard, and painful with palpation and which filled the lower half of the neck by starting from manibrium sterni and extending superiorly, was detected. In addition, there were several palpable lymph nodes in the right supraclavicular area, biggest of which was 1x2 cm in size. No abnormality was found in the other system examinations and the complete blood count test. In the conventional radiographic examination a mass was observed in the sternum, which had a heterogeneous density, irregular borders and which extended to the surrounding tissues by destroying the cortex. We performed the ultrasonography in order to further evaluation. In the ultrasonographical examination a solid mass having irregular calcifications was observed which was dense centrally and pushed the thyroid gland to the superior, due to the dense calcifications. However, the inferior spreads of the mass could not be clearly evaluated and a CT examination was carried out to assess the intrathoracic invasion of the lesion and its spreads to the other surrounding tissues. In the CT examination (Hitachi W550, Tokyo, Japan), which was carried out with a 5 mm slice width of to include the lower cervical region and the upper mediastinum, an expansive mass containing lytic-sclerotic areas was observed which caused destructions in the manibrium sterni and extended as far as to the thyroid gland (Figure 1 A-B). At the level of the thyroid gland the soft tissue component of the mass was observed (Figure 1B). Due to the irregular borders of the mass and because the mass caused widespread destructions in the bone, it was thought that the lesion was malignant and US-guided tru-cut biopsy with a tru-cut needle to obtain a core biopsy specimen was taken from the mass. The diagnosis of osteosarcoma was established by the histopathological examination. DISCUSSION OS is a malignant tumor originating from the mesenchymal cells having osteoblastic activity and frequently seen during the 2nd-3rd decades. It is the second most frequently seen primary bone tumor after multiple myeloma. While occasionally asymptomatic, it can cause a clinical presentation similar to osteomyelitis with painful swelling, deformity and increased temperature in the affected area. While OS may be located in places like costae, vertebrae and mandibula, the sternal location is extremely rare (1,2). The most common tumors of sternum are the metastases of lung, renal or thyroidal malignancies (1). Primary sternal tumors are quite rare. The most common primary sternal tumor is chondrosarcoma (2). In a study involving primary malignant bone tumors, it was reported that 14 of the 6498 cases were primary sternum sarcomas and that 2 of these were osteosarcomas (3). Sternal OS is usually asymptomatic but can be painful especially if it enlarges laterally towards the ribs (3). Since bone tumors often don’t have any specific radiological characteristics and benign and malignant lesions can mimic each other, diagnostic difficulties are often experienced. Osteosarcomas are radiologically characterized by appearance of osteolytic or osteosclerotic masses that show calcification (1-4). On CT it may show lytic, mixed or sclerotic pattern and mainly it is observed as an expansive mass lesion with irregular borders, which invades bone marrow by destroying the cortex (5). In our case, a tumoral formation with sclerotic areas was also observed, which started from manibrium sterni and extended up to the thyroid gland and caused destructions in cortex. The thyroid gland was pushed by the mass but esophagus, trachea and mediastinal vascular structures were normal in appearance. In addition, soft tissue component showing calcification was observed at the level of the thyroid gland. The exact cause of osteosarcoma is unknown. However, a number of risk factors are known such as rapid bone growth, genetic predisposition, and bone dysplasias including paget disease, fibrous dysplasia, and enchondromatosis. In addition, exposure to radiation is the only known as a environmental risk factor (5). However, there was no explanation why a patient of this age developed an osteosarcoma and we could not detect any risk factor in our patient. In conclusion, the sternal location of OS is very rare and may mimic some mass lesions such as sternoclavicular hyperostosis, thymoma, teratoma, lymphoma and goiter. While the CT findings of the OS lesions located in the long bones are more specific, in the sternal OS cases the CT is helpful in demonstrating the characteristics of the lesion’s, extension and relationship with the neighboring structures. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09010f1.jpg] |
| |||||||||

{kind=link}