 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
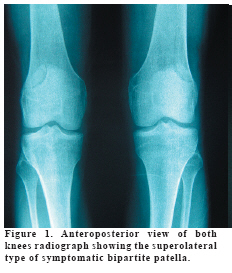
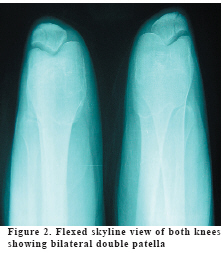
European Journal of General Medicine, Vol. 6, No. 1, 2009, pp. 52-54 An Usual Painful Bipartite Patella Ümit Dündar, Özlem Solak, Tuncay Çakır Kocatepe University Faculty of Medicine, Physical Medicine and Rehabilitation, Afyonkarahisar, Turkey Code Number: gm09012 Most bipartite patellae are asymptomatic and observed only as an incidental finding when the knee is radiographed for other reasons. Although bipartite patella is usually asymptomatic, it can become painful in subjects following overuse or injury. Most of the patients with painful bipartite patella respond relatively well to nonsurgical treatment. When the pain is persistent and resistant to those conservative treatments, a certain type of surgical procedures can be applied. In this report, we present a case of symptomatic bipartite patella in a patient with no underlying disease. Key words: bipartite patellae, anterior knee pain. INTRODUCTION Symptomatic congenital bipartite patella is an uncommon pathology. Patella is the largest sesamoid bone which ossifies from one center in 77% and from two or three centers in 23% of children (1). Most of these ossification centers fuse mutually, but approximately 2% of them remain to be dissociated (2,3) Although bipartite patella is usually asymptomatic, it can become painful in subjects following overuse or injury. Only 2% of bipartite patellae become symptomatic. It is more common in males and adolescents or young athletes but scarcely in adults and less than one-half of symptomatic cases are bilateral (4,5). In this report, we presented a case of symptomatic bipartite patella in a patient with no underlying disease. CASE A 27-year-old male who plays soccer complained of anterior knee pain both at the left and rigth sides (in the right and left knees) for 3 months, both during and after strenuous activities. He could not remember a traumatic episode preceding the initial onset of pain. However, he suffered from painful attacks at the both knees 6 months ago and he was treated only with non-steroidal antiinflammatory drug (NSAID) at another hospital at that time. The patient also reported pain when assuming a squatting position and crepitation that occurring during flexion, both of which had worsened gradually. Walking greater than 30 minutes aggravated the pain. On physical examination, there was tenderness over the superolateral portion of the both patellae. A prominent crepitus was detectable when the patient flexed his knees. No pathological finding was observed while performing following tests; McMurray test, anterior and posterior drawer tests, Apley’s distraction and compression tests, Lachman’s test, valgus and varus stress tests, Noble compression test. There were no swelling or effusion at both knees. Also, there was no limitation in the active and passive range of motion of knee joints bilaterally. Muscle strength of the lower extremities were also normal. Laboratory testing revealed that the white blood cell count, serum C-reactive protein level, erythrocyte sedimentation rate, serum calcium, phosphorus, alkaline phosphatase were within normal limits. There was a gap on the superolateral patella with corticated margins in plain radiographs of both knees. The distance between the main and accessory ossification centre was 2-3 mm. There were no additional bony abnormalities in plain radiographs of both knees. Also, there was no joint space narrowing (Figure 1 and 2). We diagnosed painful bipartite patella type III (fragment at the superolateral pole) according to Saupe’s classification based on the position of the accessory ossification center: Type I, at the inferior pole (5%); Type II, at the lateral margin (20%); and Type III at the superolateral pole (75%) (6,7). After the diagnosis of painful bipartite patella, stretching exercises of the quadriceps and hamstring muscles and strengthening exercises of quadriceps muscles were started to restore strength and flexibility of the knee joints. We started NSAID daily and also gave bilateral patellar stabilizing braces. One week later, symptoms related to bipartite patella, showed dramatic improvement. The dose of NSAID was gradually decreased and stopped in two weeks. DISCUSSION Several factors can cause anterior knee pain. The most of anterior knee pain disorders are result from patellofemoral joint abnormalities however, other pathologic conditions including injury of intraarticular structures (anterior and posterior cruciate ligaments, meniscal lesions etc.). Osteoarthritis, osteochondritis dissecans, Osgood-Schlatter disease, Sinding-Larsen-Johanson disease, synovial plica, iliotibial band syndrome, medial collateral bursitis and prepatellar bursitis, inflammatory rheumatic diseases (juvenile rheumatiod arthritis, seronegative spondiloarthropathies, etc.), neoplasms and infections may also cause anterior knee pain (8). Most bipartite patellae are asymptomatic and observed only as an incidental finding when the knee is radiographed for other reasons. The natural history of painful bipartite patella is as follows: the patella normally begins primary ossification at about 5 to 6 years. Patellar primary ossification occurs centrifugally in a mass of epiphyseal cartilage. Some patellar accessory foci may present developmental variations and a superolateral accessory center is usually evident by 12 years of age. Most secondary ossification centers fuse with the patella during adolescence and some may persist into adult years (7,9). It was suggested that a painful bipartite patella might be symptomatic if non-union induced by excess tensile force applied to the superolateral patellar pole and the accessory ossification center could not be fused between the main ossification centres (7). With rare exceptions this anomaly occurs at the superolateral aspect of the patella. The lesion is usually asymptomatic, but can be associated with localized anterior knee pain (10). In our patient, except the tenderness over the superolateral part of the patella, the orthopedic and rheumatologic physical examination tests were found to be normal. Also laboratory testing parameters were within normal limits. On radiographs corticated margins help to differentiate it from patellar fracture. The typical clinical and radiological manifestations (a gap on the superolateral patella with corticated margins) led to a diagnosis of bilateral painful bipartite patella in our patients. Most of the patients with painful bipartite patella respond relatively well to nonsurgical treatment including rest, stretching exercises of the quadriceps and hamstring muscles, strengthening exercises of the quadriceps muscle and bracing to support the patella (5,11). However, long-term success is questionable because recurrence rates are fairly high. When the pain is persistent and resistant to those conservative treatments, a certain type of surgical procedures can be applied such as lateral retinacular release, osteosynthesis with or without bone graft , and excision of the fragment (1,9,12-14). In conclusion painful bipartite patellae is one of the rare causes of anterior knee pain. Most of the patients with painful bipartite patella may respond to conservative treatment modalities. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09012f2.jpg] [gm09012f1.jpg] |
| |||||||||

{kind=link}
{kind=link}