 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
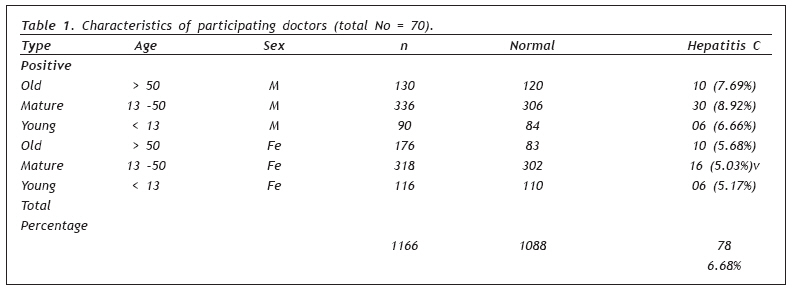
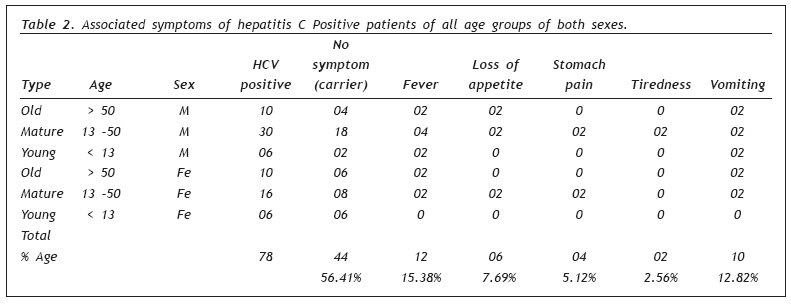
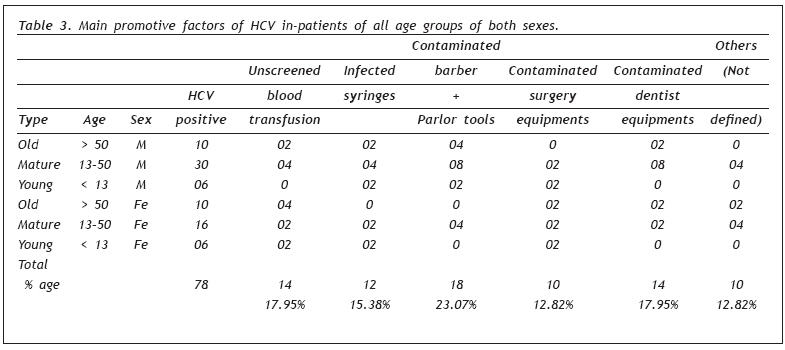
European Journal of General Medicine, Vol. 6, No. 2, 2009, pp. 94-98 Prevalence of Hepatitis C Virus (HCV) in Relation to Its Promotive Factors Among Human Urban Population of Multan, Pakistan Muhammad Ali1 , Lubna Kanwal2 , Kamran Tassaduqe3 , Rehana Iqbal4 1 PhD, Wales UK Code Number: gm09021 INTRODUCTION Hepatitis is primarily caused by infection with one of at least five different viruses, each of which has a different epidemiologic pattern of transmission, a different clinical outcome and a different mean of prevention. According to Seegar and Mason (1), Kamal (2) different viruses including hepatitis A, B, C, D, E and G cause viral infections of human liver. Hepatitis C virus was identified in 1989 when its genome was isolated from the plasma of a chimpanzee, experimentally infected with blood borne non-A, non-B Hepatitis virus. It is the most common cause of post-transfusion and community acquired non-A, non-B Hepatitis and cryptogenic cirrhosis worldwide (3). In the late 1970s, reports of primates after exposure to HCV infected human serum followed by a subsequent report of HCV infection after a needle stick injury resulted in the identification of Hepatitis C as a distinct and transmissible Hepatitis virus (4). The children and adults are at equal risk of becoming infected with HCV. An estimated 100 million individuals worldwide are chronically infected with HCV. High prevalence rates have been found in Southeast Asian countries, such as Thailand, Malaysia and India (5,6). Hepatitis C is also the most common chronic blood borne infection in the U.S. In the United States HCV causes an estimated 10,000 deaths annually (7). An estimated 20% of persons with chronic Hepatitis C virus infection develop cirrhosis over the course of 25 years. The children become infected with HCV through a variety of means including perinatal HCV infection and person to person transmission during the first five years of life. Maternal infant transmission is not common. In most studies only 5 percent of infants born to infected women become infected. The disease in newborns is usually mild and free of symptoms. The risk of maternal infant spread rises with the amount of virus in the mother’s blood and with complications of delivery such as early rupture of membranes and fetal monitoring. Breast feeding has not been linked to spread of HCV (8). The acute and chronic consequences of hepatitis C virus infection are among t he major health problems in Pakistan. Many chronically infected persons are at risk of long term sequel, such as chronic liver disease and primary hepatocellular carcinoma. Hepatitis C virus infection has different clinical manifestations depending on the patient’s age at infection, immune status and the stage at which the disease is recognized. During the incubation phase of the disease, patients may feel unwell with possible nausea, vomiting, diarrhea, anorexia and headache. Patients may then become jaundiced although low-grade fever and loss of appetite may improve. Epidemiological studies conducted in the past have provided data regarding the prevalence of HBV and HCV in different parts of the world. But few studies are available in Pakistan. The prevalence of Hepatitis C infection is high in Pakistan and nation wide efforts are required to identify people who may have been infected with HBV and HCV (9). The present study was carried out to assess prevalence of Hepatitis C virus (HCV) in relation to sex, age, promotive factors, associated symptoms and season among human urban population of Multan, Pakistan. MATERIALS AND METHODS The present study was carried out for a period of 28 months from June 2003 to October 2005. Blood samples of 556 males and 610 females of different age groups were collected randomly from the population. The male population was divided into three age groups i.e. old male (age above 50 years), mature male (age 13 - 50 years) and young male (age below 13 years). The female population was also divided into similar three groups. Efforts were made to include samples of all those persons who were willing to cooperate in carrying out the purpose of present study and were apparently normal, without any diagnosis of hepatitis C or freshly diagnosed. Blood was withdrawn by vene-puncture of arm vein. Three ml of blood sample was used for antibody titer evaluation. The estimation was carried out immediately after the collection of blood samples by using rapid chromatographic immunoassay from Acon Laboratories USA for the qualitative detection of hepatitis C surface antigen in serum or plasma. During testing, the serum or plasma samples reacts with the dye conjugate (mouse anti HCV antibody colloidal gold conjugate) which has been pre coated in the test device. The mixture migrates upward on the membrane chromatographically by capillary action to react with anti HCV antibodies on the membrane and generate a red line. Presence of this red line indicates a positive result, while its absence indicates a negative result. Regardless of the presence of HCV, as the mixture continues to migrate across the membrane to the immobilized goat anti mouse region, a red line at the control line region always appears. The presence of this red line serves as verification for sufficient sample volume and proper flow and as control for the reagents. Serum was obtained from the clot of red cells immediately after collection of blood samples to avoid hemolysis. Only clear, non-hemolyzed specimens were used. Vacuum tubes were used for the collection of serum or plasma. The HCV device used was when compared with a leading commercial RIA and EIA test of HCV the correction between these two systems was 98%. Specificity of HCV test device was also tested with laboratory strains of hepatitis A and B. They all yielded negative results. The presenting complaints, symptoms and the history of the subjects with a special emphasis on personal past history was also noted. The study was approved by the local ethical committee. RESULTS The results from the present study suggested that among the observed urban population of Multan (n=1166), prevalence of HCV was 6.68% (Table 1). The prevalence of HCV when studied in different age groups of both sexes, it was found that prevalence of HCV was maximum (8.92%) in mature males as compared to young males (6.66%) and old males (7.69%). The results suggested that among the observed female population, prevalence of HCV was higher (5.68%) in old females as compared to mature females (5.03%) and young females (5.17%) (Table 1). The predominant symptoms with HCV were elevated Bilirubin + elevated liver enzymes (17.94%), yellowish eyes + skin coloration (15.39%) and dark yellow urine +diarrhea (10.25%). The associated symptoms with HCV were fever (15.38%), vomiting (12.82%), loss of appetite (7.69%), stomach pain (5.12%) and tiredness (2.56%). The results also show that (56.41%) patients were although carrier of HCV had no symptom (Table 2). The main promotive factors for HCV were contaminated barber, parlor tools (23.07%), unscreened blood transfusion (17.94%), contaminated dentist equipments (17.94%), infected syringes (15.38%), and contaminated surgery equipment (12.82%). In (12.82%) of cases the promotive factors were not defined (Table 3). The reported cases of HCV positive patients were maximum in summer (76.92%) as compared to (23.07%) which were reported in winter. DISCUSSION Hepatitis is a public health problem worldwide. According to Gow and Mutimer (10) viral hepatitis is the major cause of chronic liver disease worldwide. The hepatitis C virus is a small, enveloped RNA virus with a positive- sense single stranded genome of approximately 9600 nucleotides. The viral nucleocapsid consists of the core protein and the viral genomic RNA enveloped by a bilayer of two glycoproteins. The HCV genome contains a single open reading frame flanked at each end by untranslated region (12-14). HCV is transmitted through percutaneous or parenteral contact with infected blood, blood products or body fluids and by sexual intercourse (12-14). In the United States before 1991, the leading mode of transmission was receipt of HCV contaminated blood transfusion due to the use of shared, unsterilized or poorly sterilized needles and syringes. However, after the introduction of routine blood screening in1990 and direct testing for HCV in 1992, transfusion related HCV infection has declined dramatically (15). With the introduction of routine blood screening in 1992 Hepatitis C has virtually disappeared. At present, injection drug use is the most common risk factor for the disease. Hepatitis C exposures among injection drug users have been reported to be higher than 50% compared to 10% in the same general population (16). Case control studies have identified other possible risk factors for the transmission of HCV including health care employment, unprotected sexual intercourse with multiple partners, low socioeconomic status, exposure to household members with a his tory of HCV, and perinatal transfer. Maternal infant transmission is not common. In most studies, only 5% of infants born to infected women become infected. The disease in newborns is usually mild and free of symptoms. The risk of maternal infant spread rises with the amount of virus in the mother’s blood and with complications of delivery such as early rupture of membranes and fetal monitoring. Breast-feeding has not been linked to spread of HCV (8). Surveys also show sexual partners of Hepatitis C patients are less than 5% infected with HCV. Testing sexual partners for anti HCV is also very important. People with multiple sex partners should be advised to follow safe sex practices, which should protect against Hepatitis C as well as Hepatitis B and HIV (8). Other known risk factors include exposure to the virus from cuts, wounds, or medical injections or procedures, ear piercing, acupuncture, tattoos, and cultural tradions involving blood contact. The use of inadequately sterilized undisposable medical materials e.g. needles and scalpels has also been shown to transmit HCV. Inadvertent needle stick injuries and lack of application of universal precautions may be contributing factors. About 80% of HCV positive surgical operation room personnel in a hospital in Pakistan had more than four needle stick injuries per year in five years (17). In one Pakistani community HCV prevalence was 6.5% and individuals who received more therapeutic injections were found to be at a higher risk for infection (18). According to Remis (19) prevalence of hepatitis is generally found highest during young and middle adulthood years. In this study hepatitis cases are found with highest prevalence among mature males of age group 13-50 years (8.92%) and old males of age group >50 years (7.69%) The results of this study also agree with the findings of Shah et al (20). They observed the highest prevalence of chronic hepatitis among the middle age group. It is a possibility that these age groups may be exposed highly to risk factors like surgery, blood transfusion, multiple injection and razor trauma of shaving. In this study the prevalence of hepatitis C is high in males (8.27%) as compared to females (5.25%) which correlates the study of Remis (19) who found that prevalence of hepatitis was higher in males than females. The reasons of this may be more exposure of males to contaminated environment, accidental cuts, razor trauma of shaving and circumcision. The extensive literature review indicates that such type of studies, which were focused to show relationship of these parameters with that of spread of HCV are rare in Pakistan. Researchers in Pakistan are stimulated to begin to identify strategies for HCV screening, medication compliance and adherence to lifestyle change recommendations. Therefore results of this study might give a wake up call to influence the attitude of physicians as well as the society towards control and prevention of these multitude factors. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09021t3.jpg] [gm09021t2.jpg] [gm09021t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}