 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
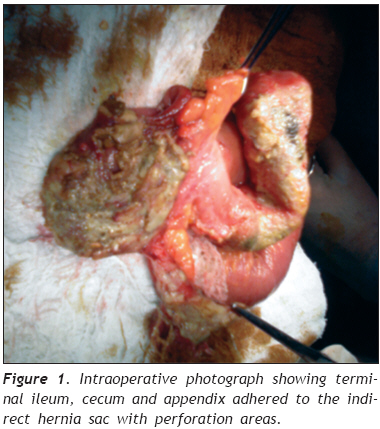
European Journal of General Medicine, Vol. 6, No. 2, 2009, pp. 116-118 Amyand’s Hernia Mimicking Acute Scrotum Fahrettin Yıldız1, Alpaslan Terzi1, Saçid Çoban2, Ali Uzunkoy1 1 Harran University Medical Faculty, Department of General Surgery Code Number: gm09025 ABSTRACT Amyand’s hernia is an inguinal hernia with an appendix involved. It is a rare condition. Perforated appendicitis is much less common in this situation and very few cases have been reported in the literature. Preoperative diagnosis is difficult. If additional pathologies exist, the diagnosis is more troublesome. We aimed to present a patient with Amyand’s hernia mimicking acute scrotum which is rare in the literature. Keywords: Amyand’s hernia, acute scrotum, appendicitis. INTRODUCTION Amyand’s hernia is an eponymous disease named after Claudius Amyand, who performed the first successful appendectomy in 1735 (1). This condition is a rare form of inguinal hernia with an appendix involved and may become incarcerated. The incidence of having a normal appendix within the hernial sac varies from 0.5% to 1%, whereas only 0.1% of all cases of appendicitis present in an inguinal hernia, underscoring the rarity of the condition (2). Amyand’s hernia is commonly misdiagnosed as an ordinary incarcerated hernia. Symptoms mimicking appendicitis may occur. In cases of appendical inflammation or perforation, treatment consists of a combination of appendectomy and hernia repair. Placement of prosthetic mesh materials for hernia repair in the presence of pus or perforation is not recommended due to a high rate of chronic wound infection, mesh sepsis, extrusion and fistulae (3, 4). We report a case of Amyand’s hernia with giant hydrocele in a 75-yearold man. CASE REPORT A 75-year-old man with a progressive pain in the right lower quadrant and scrotum for 48 hours, was referred to the general surgery department. He was also suffering from nausea, emesis, anorexia and constipation. He had a past medical history of irreducible inguinal hernia with a bilaterally giant hydrocele for 10 years. Physical examination on admission revealed a tender and non-reducible mass in scrotum. He had generalized peritoneum irritation signs as well. Serum laboratory values were unremarkable with the exception of a leukocytosis (white blood cell count [WBC], 25,000/µm3[Normal values: 4300-10300 µm3]). Bilaterally giant hydrocele and right sided intestinal loops with purulent content in scrotum, was revealed by ultrasound. The American Society of Anesthesiologists (ASA) grade was IV. The diagnosis of incarcerated right inguinal hernia was established and the patient was scheduled for surgery. A broad spectrum intravenous antibiotic (piperacillin/tazobactam) was administered in preparation for surgical exploration. Surgery was carried out approximately 6 hours after the initial assessment and preparation of the patient with the diagnosis of incarcerated inguinal hernia. Right inguinal oblique incision was performed for exploration. At surgery, an incarcerated inflammatory and edematous mass was found inside the scrotum with stench. This mass was identified as the terminal ileum, cecum and appendix adhered to the indirect hernia sac with perforation areas at cecum and appendix (Figure 1). Ileo-cecal resection with end ileostomy was performed. Modified Darn repair, described by Zeybek et al. (5) was applied for the defect. A vacuum drainage was left in scrotum and it was removed at the postoperative fifth day. The postoperative course was devoid of important occurrences, and the patient was discharged in good condition within 7 days. Histopathologic examination showed perforated appendicitis with periappendicular abscess, and caecal perforation. DISCUSSION The term Amyand’s hernia is used for depicting the condition of non-inflamed appendix, inflamed appendix or perforated appendix within an inguinal hernia (6). The Amyand’s hernia in adults is rare and incidence of this condition is approximately %1, association with perforated appendicitis is even rarer (7). Its accurate diagnosis can be substantiated only with high clinical suspicion, since the symptoms associated with this disease state vary considerably. The most common clinical presentation involves rapidly progressing tenderness over a previous external hernia site, evocative of a strangulation or incarceration in the absence of radiographic evidence of obstruction (8). Only one case has been reported which was correctly diagnosed preoperatively in 60 cases of Amyand’s hernias from 1959 to 1999 (9). In the emergent conditions, differential diagnosis should include strangulated or obstructed hernia, strangulated omentocele, Richter’s hernia, testicular tumor with hemorrhage, acute scrotum, inguinal adenitis and epidydimitis (2). In the presence of appendicitis or perforation of appendix, the majority of the reported cases have had similar symptoms with an obstructed or a strangulated hernia. Hence, preoperative diagnosis of Amyand’s hernia is so difficult. If there is an additional disease, such as hydrocele or epididymitis, diagnose becomes more difficult. To the best of our knowledge this is the first case of Amyand’s hernia with an additional disease. In this case, the initial treatment was started by urology department as an acute scrotum. After the constancy of the symptoms, the patient was referred to our clinic. So the treatment was delayed. The present case of Amyand’s hernia is diagnosed during surgery. Acute appendicitis occurred over the body of the appendix located in the scrotum together with cecum and terminal ileum. Weber and colleagues presumes that the inflammatory swelling may lead to incarceration, subsequent impaired blood supply (9). The pathological mechanism of appendicitis in cases of Amyand’s hernia is still a controversial subject. It may be due to inflammatory swelling but the size of the deep ring and the amount of content protruding through it, which causes strangulation may play an important role. Despite the presence of inflammatory swelling, the blood supply was not affected and strangulation did not develop in our case. The body of the appendix appeared to be perforated and cecal perforation was probably developed secondary to this. Fecal content and pus formation was also found inside the scrotum. Since the patient was unstable at the time of the operation, we preferred to perform ileocecal resection with end ileostomy. We repaired the hernia by the modified darn method described by Zeybek et al. to prevent the possibility of infection by the insertion of a mesh (5). Controversy about the hernia repair of the infected area still exists and mesh is not suggested in the contaminated abdominal wall defects because of the greater risk of wound infection and appendiceal stump fistula (2). To repair hernia, modified darn method can be carried out in such cases by using a drain. We are reporting this case for its rarity of occurrence, especially perforated appendix within an inguinal hernia. Awareness of this condition would be useful in the preoperative evaluation of patients with hydrocele, non-reducible or incarcerated inguinal hernias. The presence of pus or perforation of the appendix may be a contraindication to the placement of a mesh for hernia repair if biodegradable mesh is not available. Modified darn method may become a choice in the surgical repair of hernia defect in the presence of pus or perforation. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09025f1.jpg] |
| |||||||||

{kind=link}