 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
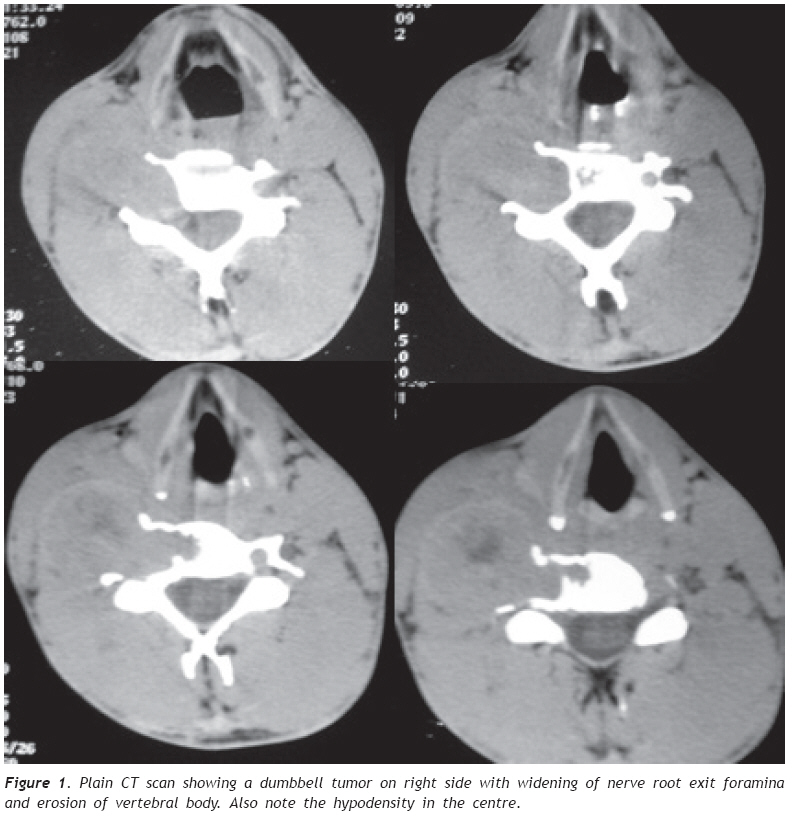
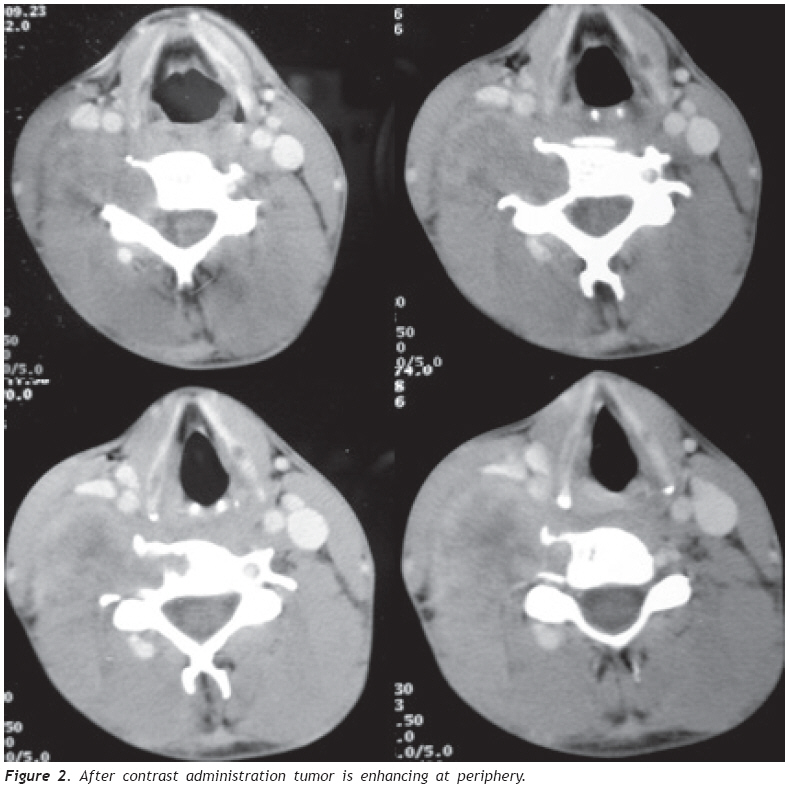
European Journal of General Medicine, Vol. 6, No. 2, 2009, pp. 123-126 CT Characteristics of Dumbbell Schwannomma Arising From The Fifth Cervical Nerve Root Amit Agrawal1, G.K.Singh2, Raj Kumar Rauniyar3, Ishwar Singh4, Sangeeta Shrestha5, Rajat Agrawal6 1 Consultant Neurosurgeon, Department of Surgery, B.P. Koirala Institute of Health Sciences, Dharan, Nepal 2 Professor in Orthopedics, Department of Orthopedics, B.P. Koirala Institute of Health Sciences, Dharan, Nepal 3 Additional Professor in Radiology, Department of Radiology, B.P. Koirala Institute of Health Sciences, Dharan, Nepal 4 Professor in ENT, Department of ENT, B.P. Koirala Institute of Health Sciences, Dharan, Nepal 5 Assistant Professor in ENT, Department of ENT, B.P. Koirala Institute of Health Sciences, Dharan, Nepal 6 Assistant Professor in Surgery, Department of Surgery, B.P. Koirala Institute of Health Sciences, Dharan, Nepal Code Number: gm09027 ABSTRACT Neurilemmomas, or schwannomas, are benign neurogenic tumors that arise from the nerve sheaths of peripheral nerves. Neurilemmomas may occur nearly anywhere in the body but have a predilection for the head, the neck, and the flexor surfaces of the upper and lower extremities. Histopathology is the most definitive way to confirm the nature of these lesion, however well planned CT scan will adequate pre-operative information for surgical planning. Though MRI is the gold standard and investigation of choice well planned thin sliced CT scan can be is as good as MRI for the pre-operative evaluation of these lesions. Key words: Neurilemmoma, CT scan. INTRODUCTION Neurilemmomas, or schwannomas, are benign neurogenic tumors that arise from the nerve sheaths of peripheral nerves. They tend to be encapsulated, with the nerve fibers stretched around the tumor. Neurilemmomas may occur nearly anywhere in the body but have a predilection for the head, the neck, and the flexor surfaces of the upper and lower extremities. (1) In this case report we discuss CT scan findings in a case of cervical dumbbell neurilemmoma. CASE REPORT Thirty years old male presented with progressively increasing swelling on right side of neck for 1 year duration. It was associated with radicular pain, paresthesia and weakness at right shoulder abduction. On physical examination he had grade 4/5 weakness of right shoulder and sluggish right biceps jerk. There were no other deficits. A non-tender, mobile, and firm mass was detected on physical examination on right side of neck. Skin over the mass was freely and there was no ulceration. Thin sliced CT scan showed a well defined dumbbell shaped mass located in the and weakness of right shoulder weakness was worsright neuronal foramina causing foraminal widening and bony destruction (Figure 1 and 2). The lesion was enhancing at periphery after contrast administration (Figure 2). All these imaging findings including dumbbell configuration were suggestive for peripheral two different components, designated by the Swedish neurilemmoma. The mass lesion was removed totally. Part of the tumor which was extending deep into are highly cellular and are composed of spindle cells the nerve root exit foramina could not be removed. During the procedure nerve root could not be saved and weakness of right shoulder weakness was worsened. DISCUSSION Histopathologically neurilemmomas usually consist of two different components, designated by the Swedish neurologist Nils Antoni as A and B. Antoni type A areas are highly cellular and are composed of spindle cells that often have a palisade or organoid arrangement. In Antoni type B areas, the tumor cells are separatedby abundant edematous fluid that may form cystic spaces (2). Inadequate blood supply to the center of the tumor sometimes causes secondary degenerative changes such as cyst formation, calcification, hemorrhage, and hyalinization (1). In this case report we discuss the CT characteristics of dumbbell cervical neurilemmoma. As in the present case on CT scan, a neurilemmoma appears as a well-demarcated round or oval mass that frequently demonstrates prominent cystic degeneration and calcification. Calcifications are punctate, mottled, or curvilinear and are seen along the walls of the mass. At contrast-enhanced CT,neurilemmomas demonstrate variable homogeneous or heterogeneous enhancement. Heterogeneous contrast enhancement represents variation in the degree of cellularity. Loose cellularity with diffuse edematous change may result in minimal contrast enhancement as in the present case. Heterogeneous areas on enhanced CT scans may also be due to cystic and hemorrhagic changes (3-5). Neurilemmoas need to be differentiated from neurofibromas. Although both neurilemmomas and neurofibromas are of nerve sheath origin, each has a characteristic histological appearance and can occur in different clinical settings. Unlikeneurilemmomas, neurofibromas are not encapsulated and lack a clear partition into Antoni A and B areas. Nerve fibers run through neurofibromas; this finding also helps distinguish them from neurilemmomas, in which the nerve fibers diverge and course over the surface of the tumor before reconverging distally to form a normal nerve. In addition, in contrast to neurilemmomas, pure neurofibromas are solid tumors at macroscopic analysis. Areas of cystic degeneration, hypocellularity, and xanthomatous material are uncommon in neurofibromas. Neurofibromas often undergo malignant degeneration, particularly in cases of neurofibromatosis, whereas neurilemmomas rarely if ever undergo malignant degeneration. Neurofibromas occur more frequently in men than in women. They are commonly diagnosed in patients in the 2nd to 4th decades of life. On CT scan, neurofibromas have a homogeneous, smooth, round appearance with distinct outlines. They have attenuation values of 20–25 HU on unenhanced scans as well as homogeneous enhancement with attenuation values of 30-50 HU on contrast-enhanced scans (6). Neurofibromas often contain multiple cystic spaces of varying size that are caused by myxoid degeneration. At CT or MR imaging, neurofibromas and schwannomas occasionally demonstrate a target-like enhancement pattern, with different attenuation or signal intensity in the central portion than at the periphery. Histopathology is the most definitive way to confirm the nature of these lesions. MRI is the gold standard pre-operative investigation, however a well planned CT scan will provide adequate pre-operative information for surgical planning. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09027f2.jpg] [gm09027f1.jpg] |
| |||||||||

{kind=link}
{kind=link}