 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
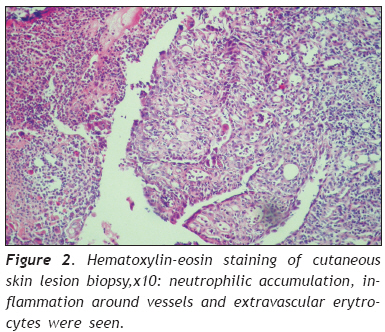
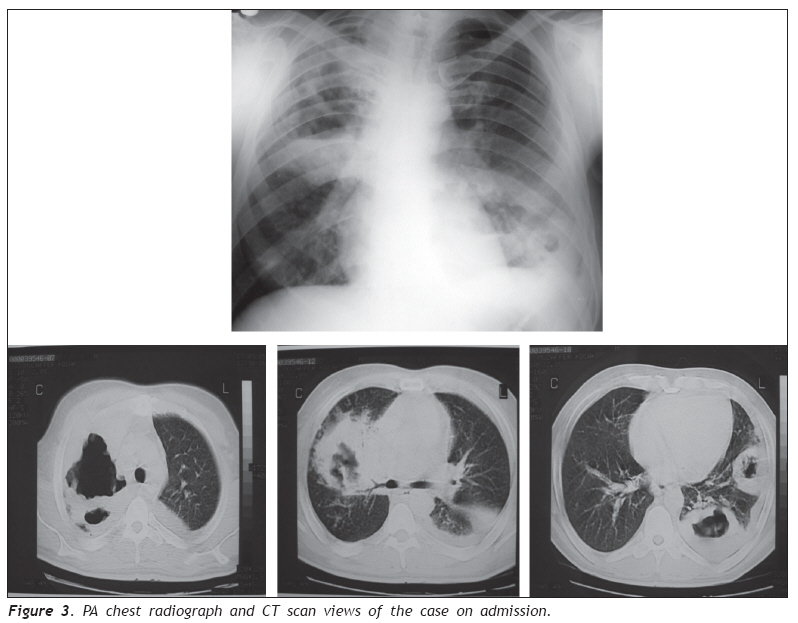
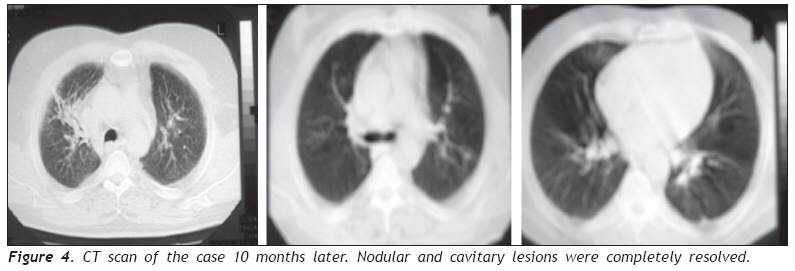
European Journal of General Medicine, Vol. 6, No. 2, 2009, pp. 131-135 Pyoderma Gangrenosum Presenting with Pulmonary Cavitary Lesions Şebnem Yosunkaya1, Hatice Toy2, Emine Genç3, Bengi Akın1, Emin Maden1, Faruk Özer1 1 Selcuk University, Meram Medical Faculty, Department of Pulmonary Medicine, Konya, Turkey Code Number: gm09029 ABSTRACT Neutrophilic dermatoses like pyoderma gangrenosum (PG) are characterized by sterile, neutrophilic, cutaneous infiltrates. Extracutenous neutrophilic infiltrations may also be seen, but pulmonary involvement is very rare and usually characterized by patchy infiltrates or interstitial pneumonitis. In this case, a PG case who had cutenous lesions and large cavitary lung nodules, is reported. He was a 49 years old male patient whose thorax computed tomography revealed multiple pulmonary nodules with central necrosis. In his transbronchial and bronchial biopsies, nonspecific inflammatory aseptic nodules were detected corresponded to the pathologic findings of skin lesion biopsies. A dramatic response was occured after applying corticosteroid and immunesupressive treatment. In conclusion, cavitary pulmonary nodules of our case were thought to be due to pulmonary involvement of PG. Key words: Pyoderma gangrenosum, lung, cavity. INTRODUCTION Pyoderma gangrenosum (PG) is a rare skin disease with unknown etiology. Usually systemic involvement is also seen in association with cutenous involvement. Histologic examination reveals significant neutrophilic infiltration in dermis. Although it is commonly associated with inflammatory bowel disease, arthritis, and immunologic and hematologic diseases, PG may also be seen in normal hosts (1,2). Lesions are often limited to the skin, but sterile neutrophilic infiltration can occur in lung, heart, central nervous system, joints, gastrointestinal tract and eyes as well (3). So far, only two cases presenting with cavitary lesions has been reported in the literature (4,5). CASE REPORT A 49 years old male patient was presented to our clinic with the complaints of fever, productive cough, hemoptysis, fatique and ulcerative painful lesions on his extremities. His past medical history revealed previous hospitalizations in different hospitals due to complaints of cough and sputum production. These complaints started 3 months ago. In his thorax compute tomography (CT), there were multiple cavitary nodules in right and left upper lobes. The diameter of the nodules were 9 cm, 6 cm and 3.5 cm. Bronchial biopsy done at these hospitals revealed nonspecific inflammatory aseptic necrosis. Acid fast bacillus (AFB) was negative both in lavage and tissue cultures. The patient received non specific empirical antibiotic therapy in the first clinic he was hospitalized. In the second clinic he went one month later he was started empirical tuberculosis therapy including rifampicin, pyrazinamide and isoniazid despite his sputum smear for AFB was negative. There was no clinical or radiological improvement eventhough he had taken this therapy for two months. While he was receiving this therapy he had lost 15 kg of weight. Two months before he admitted to our clinic, painful skin lesions were appeared on his extremities. His third hospitalization to a hospital was due to subarachnoid hemorrhage 17 days before admission to our clinic. He was admitted to that hospital with complaints of headache, dysarthria and imbalance. There was no history of head trauma, but his cranial CT demonstrated subarachnoid hemorrhage. Clinically, he got better with supportive treatment and was referred to our hospital for evaluation of pulmonary lesions. In his family history nobody had similar symptoms. He has a 30 pack/year smoking history. In his physical examination fever was 39,4°C, heart rate 90/ min and blood pressure was 120/70 mmHg. There were painful, ulcerative papulonodular skin lesions on extensor surface of his hands, wrist, arms, heels, ankles and on the fingers of hands and foot (Figure 1). The lesions on his ankle and wrist were bigger and deeper with sizes of 3x1 cm, others were 1 cm in size. There were also painful white and yellowish nodules on his lip, pharyngeal and cheek mucosa. His chest examination revealed fine rales at the bottom of right lung and decrease in breath sounds at the superior of right lung. Other physical examination findings were unremarkable. The biopsy result of the lesion on the dorsum of the right hand revealed neutrophilic dematoses which was concordant with PG (Figure 2). The pathology of transbronchial and bronchial mucosa biopsy were reported as chronical nonspecific inflammation. Laboratory investigation demonstrated leukocyte value of 17,600/mm3, hemoglobin 9,6 g/dL, hematocrit 28%, thrombocyte 329 × 103/mm3 and reticulocyte value of 0.2%. Differential cell count revealed 55% polymorphonuclear leukocytes, 20% band cells, 20% lymphocytes, 5% monocytes, and %2 eosinophils. Erythrocyte sedimentation rate was 120 mm/h. Hepatitis antibodies, serum protein electrophoresis, complement level and autoantibodies such as ANA, c-ANCA were all normal or negative. The diameter of tuberculin skin test was 10 mm. Peripheral blood T total, T helper, T cytotoxic, B ve Natural killer cells were within normal limits. HIV antibody was negative with enzyme-linked immunosorbent assay. Arterial blood gas analysis findings were: pH: 7.48, PaO2: 67.9 mm Hg, PaCO2: 29.7 mm Hg and SaO2: 94,8. Biochemical analysis results were: C reactive protein (CRP) level: 18mg/dl (normal level <2.5 mg/ dl); protein electrophoresis: albumin 33% (range 5363), 1 10,8% (1,5-4,5), 2 19,4 (6-12), 12,3% (1117), 24,5% (12-20); IgG 14.1 g/l (8.0-17.0), IgA 2.73 g/l (1.0-4.9) and IgM 0.82 g/l (0.5-3.2). Complete urinanalysis was normal. His chest radiograph demonstrated pneumonic infiltration including cavitery lesions in both upper lobes. In his thorax CT scan, consolidations with central cavitation and abscess in the right upper, middle lobes and left upper lobe were detected (Figure 3). Blood, urine, throat, skin lesions and sputum cultures were negative for mycobacteria, nocardia and fungus and no pathogenic microorganism grew in the culture. No pathology was seen in two-dimensional transthoracic echocardiographic, especially no evidence of valvular vegetations. In sinus CT scanning, paranasal sinuses and nasal cavity were normal. There was no finding about renal pathology which is the frequently involved organ in Wegener’s granulomatosis (WG). Fiberoptic bronchoscopy investigation revealed diffuse white, yellowish mucosal nodules involving trachea, right and left bronchial system and enlargement in blood vessels of the mucosa. These lesions were similar to lesions in oral mucosa. No pathogen was detected in the microbiological evaluation of bronchial lavage. Histopathological examination of tracheal lesions showed neutrophil and monocyte infiltration, but no vasculitic or granulomatous characteristics. After the diagnosis of pyoderma gangrenosum had been done, all ampiric medications of the patients was stopped. Intravenous prednisolone 500 mg/ every other day and azathioprine 150 mg/day treatment was initiated for a week. Afterward the treatment was continued with 60 mg/d oral prednisolone and 150mg/day azathioprine. The clinic and skin lesions of the patient began to improve significantly in 10 days. Oral prednisolone was stopped after 8 weeks by reducing the dose 8 mg/kg every week, azathioprine was continued with the same dose. Two months later while he was externated, his skin lesions and oral mucosa lesions were completely healed and he had no complaint. Cavitary lesions were still present in his chest CT, but the sizes were smaller and the wall of the cavity became thinner. In his chest radiograph there was only minor residual infiltrations. Nine months later his thorax CT revealed only a fibrotic sequela in the right upper lobe, other lesions were completely disappeared (Figure 4). DISCUSSION PG is a disease of unknown origin, but it is thought to be due to immune system dysfunction and/or improper functioning of neutrophils (1). It is usually In neutrophilic dermatoses, extracutenous neutroseen in association with systemic diseases such as philic infiltrations may involve lungs, bones, joints, inflammatory bowel disease, hematological diseases, central nerveus system, lymph nodes, spleen, gastroautuimmune diseases, and in some cases with trauma. intestinal system, blood vessels and eyes (2). Twenty None of these disorders were present in our case. four patients with neutrophilic dermatoses who had culture negative pulmonary lesions were reported in literature (5-8) Cavitery pulmonary lesions were reported in only two cases (4,5). Pulmonary lesions usually exists concurrent with skin lesions or later but in our case, pulmonary lesions developed before skin lesions. In our case, an infectious etiology, especially tuberculosis was thought in diagnosis, but presence of skin lesions made us to think of a systemic disease. Due to no response to empirical tuberculosis treatment we ruled out tuberculosis. AFB was negative in his sputum and bronchial lavage examination. Also no pathogenic microorganism grew in his urine, blood and throat cultures and culture of skin lesion, but presence of nonspecific inflammation predominat with neutrophils in skin, bronchial and transbronchial biopsy samples that were sent to pathologic examination made us to think of PG as a probable diagnosis. The response to corticosteroid and immunosupressive treatment in a short time confirmed the diagnosis. The most common disease that necrotic nodule occur in lungs is WG and the disease that differential diagnosis should be done with PG, is also WG. The characteristic clinicopathologic finding of WG is a necrotising granulomatous vasculitis. In our case, there was no finding of granulomatous inflammation including necrotising vasculitis in bronchial mucosa or transbronchial lung biopsies that were repeated several times. Skin lesions were seen nearly in 45% of WG cases, biopsy samples of skin lesions frequently reveal vasculitis with or without granulomatous in flammation. Rarely, features similar to PG may be seen (10). Pulmonary involvement is seen nearly in all cases with WG besides this, kidneys, joints, upper airways and sinuses are frequently involved. But granulomatous lesions with regard to renal and upper airway involvement, which are frequently involved areas, were absent in physical examination and CT scan. There were no vegetations in heart that may be seen in WG. pANCA may be positive in PG, but cANCA developes directly against PR3 and its highly suggestive of WG (11). Eventhough pulmonary lesions were radiologically similar to lesion of WG, as cANCA is negative in our case, we excluded WG. The skin lesions were healed completely with therapy. Surgical debridement is recommended for patients whose lesions do not resolve completely (12). In conclusion, we described a PG case with typical ulcerations associated with cavitary pulmonary nodules. Histopathologically it was showed that the lesions were in the form of sterile neutrophilic infiltrations. Investigations with regard to infectious etiologies were negative. Probably previous complaints and hospitalizations due to pulmonary lesions were because of a neutrophilic process, because there was no evidence of bacteriological etiology and no response to antibiotic therapy. Progression was occured in pulmonary nodules and cavitary lesions during antibiotic treatment, but pulmonary and cutaneous lesions had improved substantially with corticosteroid and immunosupressive therapy. REFERENCES
Copyright 2009 - European Journal of General Medicine The following images related to this document are available:Photo images[gm09029f4.jpg] [gm09029f1.jpg] [gm09029f3.jpg] [gm09029f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}