 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
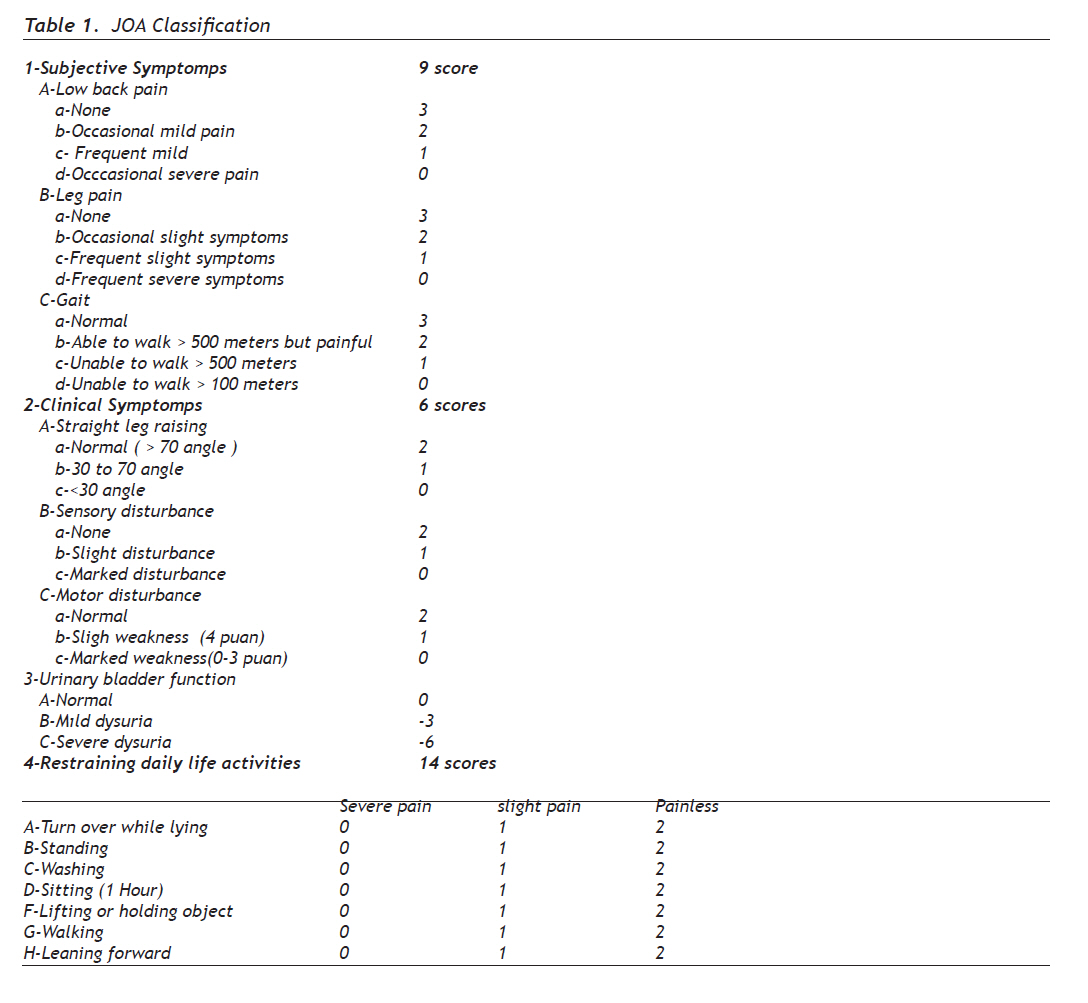
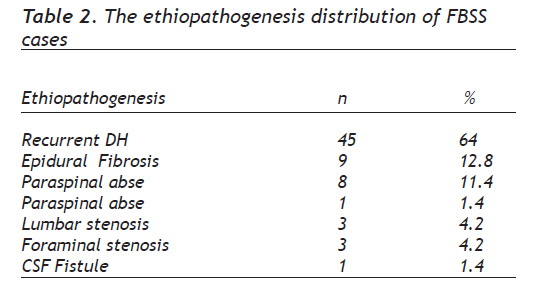
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 130-135 Original Article Failed Back Surgery Syndrome in Lomber Disc Herniation: The Retrospectıve Analysis of Success Scorings of Epidural Fibrosis and Recurrent Cases in Reoperations Lomber Disk Herniasyonunda Başarısız Bel Cerrahisi; Epidural Fibrozis ve Nüks Olgularının Reoperasyondaki Başarı Skorlamasının Retrospektif İncelenmesiMetehan Eseoğlu1, Hidayet Akdemir2 1Kilis State Hospital, Specialist of Neurosurgery, Kilis-Turkey Correspondence: Op.Dr.Metehan Eseoğlu, Kilis State Hospital/ KİLİS, GSM: 0505 679 10 88 and 0533 311 19 57, E-mail: metehaneseoglu@gmail.com Received: 12.04.2009 Accepted: 10.08.2009 Code Number: gm10025 ABSTRACT Aim: In this work, failed back surgery syndrome(FBSS) which observed in Lomber disc herniation(DH) postoperatively is analysed; and especially epidural fibrosis and recurrent cases are retrospectively analysed through calculating the success scores. Key words: Failed back surgery, recurrent disc herniation, epidural fibrosis Amaç: Bu çalışmada Lomber DH cerrahisi sonrası görülen BBC, özellikle epidural fibrozis ve nüks olgularının reoperasyondaki başarı skorlamaları yapılarak retrospektif olarak incelenmiştir. Anahtar kelimeler: Başarısız bel cerrahisi, nüks disk hernisi, epidural firozis INTRODUCTION This problem usually observed in people between 40-50 ages; especially the ones, working for industry and services sector encounter low back pain more (2). In the USA 7 million new low back pain sufferer appear each year and 200.000 of them are applied Lomber spinal surgery. 20% of them are reoperated by reason of lasting pain (1). Among the all low back pain types, the 2-3% develop by reason of Lomber Disc Herniation (DH) (3). New developments in the area of diagnostic testing methods serve much to raising diagnosis rates of lomber DH and also thanks to new technological improvements, surgical methods vary and develop (4). In the USA 200.000 people operated by reason of Lomber DH in a year and this fact implies the significance of retrospective and prospective studies to be carried out for this type of surgery. Lomber DH is mostly seen in middle aged people . While 70% of all cases are of 30-50 ages, 10% of them meet the disease after sixty years (5). However Lomber DH is rarely seen in early ages (6). 15% of all Lomber DH are applied surgical methods. Although the surgical success rate is about 90% in lomber DH many studies in literature were carried out in order to find out what sort of treatment plan should be developed for the patients whose pain still come to no end (7,8). Although these hard studies, there is no standardized approach or operation procedure formed for failed back surgery syndrome(FBSS) (7). Despite it changes among the series; today, the incidation of recurrent Lomber DH is announced as 4 %. MATERIALS AND METHODS We researched 1268 Lomber DH cases in total, operated in second brain surgery clinic in Prof. Dr Mazhar Osman Bakirkoy Ruh Sagligi ve Sinir Hastaliklari Hospital in January 2000–December 2006. 1145 cases were included to the study that were operated in our clinic and visited us for being checked regularly. 123 cases were not studied because they did not come for being checked. Among the all cases included to the study 70 cases were evaluated as FBSS and analysed retrospectively. FBSS were accepted as the cases which were in worse condition than their former preoperation status or were not better postoperatively. Radiological diagnostic examination methods, such as; direct lomber graphies, dynamic graphies for the ones who would have suffered from instability or pars defect, ( flexion, extansion and normal lomber graphies), Computerized tomography (CT) and Magnetic Resonans Image (MRI) were applied to all cases before surgery. It was aimed to have an idea about the bone area; hemylamynotomy, hemylamynectomy, laminectomy, taken in the former surgery; and especially facet joints (facet hypertrophia, medial facetectomy, total facetectomy) examined carefully. Through Lomber MRI examination; fibrosis existence or absence was searched especially in the image with contrast fluid; it was questioned if there was recurrent herniation or not; Cerebro Spinal Fluid (CSF) existence or absence related to dural damage were carefully analysed, it was searched if there were materials related to disc infection or not . The cases with DH on the same or opposite side of primer DH level were assessed as relapse. The age, sex, radiological and clinical diagnosis, surgical enterprise techniques, examination materials, operation notes of FBSS cases were analysed retrospectively. Japanese Orthopaedic Association (JOA) Scoring (9) was used for evaluation of preoperative clinical symptoms of the FBSS cases (Table 1). The evaluation of surgical result was made according to the preoperative and postoperative JOA scores comparision. Surgical Assessment: (postop JOA score – preop JOA score) / (29- preop JOA score) x100%. In our study, statistical analysis of cases Student-T and Ki Square ( x2) were used in SSPS computer programme. RESULTS Of all the cases; 36 were women (51.4%) and 34 were male (48.6%). Ages change from 22 to 74 and average of ages was 49.9. The onset of symptoms of FBSS cases changed from 15 days to 48 months; and the average was found as 8 months. We analysed 70 cases in total that were operated because of FBSS. The 45 (64%) were of recurrent DH, 9 (12.8%) epidural fibriosis and recurrent DH, 8 (11.4%) paraspinal abse, 1 (1.4%) postoperative discitis, 3 (4.2%) lomber stenosis, 3 (4.2%) foraminal stenosis, 1(1.4%) CSF fistule (Table 2). The cases with recurrent DH were to be reoperated and to achieve this former hemylamynectomy area was partially widened and then discectomy and foraminotomy were applied. When the cases who were operated by reason of recurrent DH analysed, it was observed that 26 (37%)of patients operated by left L4-L5 distance, and 17 (24.2%) right L4-L5, 8 (11.4%) left L5-S1, 10 (14.2%) left L5-S1, 4 (5%) right L3-L4, 4 (5%) left L3-L4 and 1 (1.4%) L2-L3. Postoperative success rate analysis of the FBSS cases, is done by taking sexes into consideration; as a result, 66.28% was reported for male patients and 66.98% was reported for women. The statistical comparison of the rates was meaningless (p>0.05). Success rate according to the JOA scoring; was found as 37.3% for the cases with epidural fibrosis. For the cases with recurrent DH the success rate was %75.9. Statistical comparison was found as meaningful. (p<0.05) (Table 3) DISCUSSION T However there is no acurrate definition of failed back surgery syndrome, there are many expressed in literature. According to a definition on which many neurosurgeons agree; FBSS is mentioned on the condition that back surgery fails to meet expectations, objectives and aims of a patient before the operation (10). However FBSS is accurately mentioned for the patients whose condition is worse than primer preoperation status, or who cannot reach better condition. In 1981, Burton and his friends expressed that they found the reasons of FBSS as; 58% lateral stenosis, 7-14% central stenosis, 16% recurrent DH, 6-16% aracnoidit and 6-8% epidual fibrosis (11). Fritch and his friends reoperated 136 cases with FBSS after classic laminectomy and discectomy and they expressed that in those 136 cases in total; 62% were with recurrent DH; 23% different level DH, 12% instability, %5 fibrosis (12). In our study, in 45 patients of all FBSS cases, recurrent DH was fixed as the reason of FBSS (64.2%). Literature contains different views on definition of recurrent DH. Recurrent DH is expressed as the development of DH, on the same level, same part, or on the opposite part (13, 14, 15). Some other researchers defined different-level herniation as recurrent DH (16). The major complaint of the cases in our study was radiculer pain. 10 cases had neurological intermittan cladication. It is stated that; this clinical symptom; the radiculer pain, develops as seconder the spinal canal degeneration (17). Long lasting studies on recurrent DH indicate that many different factos effect prognosis. In Finnegan and his friends’ study it is expressed that symptoms which occur less than one year or six months have better prognosis (18). Some writers indicate that, in recurrent DH, there is no need to additional discectomy, only the removal of extrude DH is enough (19). However Baba and his friends Express that anulus and nucleus have to been removed as much as possible (20). It is also stated that radical discectomy decreases disc function and lead patients experience postoperative back pain more (19). Epidural fibrosis is detected as the second FBSS cause (12.8%) in our study. While the success rate of the cases with epidural fibrosis is 37.4%, it is 75.9% in the cases of recurrent DH without fibrosis. This fact points out that success rate is decreasing in the cases that are operated after the fibrosis tissue occured. On this account, in the radiological examination; the FBSS cases with noticable epidural fibrosis formation must be well assessed prior to operation. In the analysis of Lomber MRI with contrast fluid; the distinction between epidual fibrosis and recurrent DH is made about the rate 89%. Braveman and his friends reported that, in the cases they operated by reason of epidural fibrosis, the success rate was reported as 30-35%. It was also reported that they fixed bad result in 10- 20% of the cases (21). After lomber discectomy, different level epidural fibrosis developed in almost all cases. As wound healing happens fibrotic tissue occurs instead of epidural adiposit tissue (22). The semi-fluid structure of epidural adiposit tissue helps dura and nerve roots smoothly and regularly move with spine without straining or compression.The loss or decrease of epidural adipocit dokusu after lomber disc surgery and the formation of epidual fibrosis causes straining and compression in dura and nerve root. Many materials and procedures were developed in order to prevent fibrosis formation after lomber discectomy. One of those methods is usage of otogreft adiposit tissue (23,24). But the histiological differences between epidural and subcutaneous adiposit tissue lead to take dissatisfying results (25,26). In some studies it is stated that usage of minimal invasive surgery methods and, meticulous and very careful supplication of hemostasis decrease the formation of epidural fibrosis (26). Another study states that, powder in surgery gloves and cottons that are put in the epidural area take role in the formation of epidural fibrosis (27). Many synthetic materials are also tested in order to checking the epidural fibrosis after lomber surgery.(28,29) In the comparative experimental studies; it is reported that Vicrly Mesh prevent epidural fibrosis (30). Some studies claim that through the usage of ADCON-L synthetic material, postoperative fibrosis formation can be prevented (31).However it is reported that through the usage of ADCON-L, CSF leak was observed (32,33). In Ozer and his friends’ study, the protection of ligamantum flavum throughout the operation, meaningfully decreased epidural fibrosis (22). Foraminal stenosis is another FBSS reason that is found out in our study. 6 (8.4%) of 70 cases were reoperated because of foraminal stenos. In Burton and his friends’ study, the foraminal stenosis rate was reported as 57-58% (11). In Waguespack and his friends’ study this rate was reported as 29% (10) Postoperative discitis and paraspinal abse were detected as other reasons of FBSS. Infection was observed in 10 (13%) of all cases in our series. stafylococus aureus was produced bacteriologically in the two of the cases who have postoperative discitis and paraspinal abse. Although postoperative discitis was reported to be observed as 0-3% in different series prior MRI, it was reported that, this rate observed to be increased with the common usage of MRI. In conclusion, recurrent disc herniation; which occur on the same level, the same side or opposite side , is the most frequently observed (64%) reoperation cause in the patients on whom Lomber DH surgery applied. Epidural fibrosis formation is secondly frequent cause (12.8%) of reoperation. While the success rate of all failed back surgery syndrome cases is found as ; 37.3% for the patients with epidural fibrosis and 75.9% is reported for the patients without fibrosis. The statistical comparison is found as meaningful of these success rates.(p<0.05). Therefore , the cases with epidural fibrosis have to be well-assessed radiologically and clinically ,and the best treatment plan should be aimed and formed.In order to prevent epidural fibrosis ; minimal invasive surgery techniques have to be applied and careful hemostasis is to be supplied. ACKNOWLEDGMENT I am so grateful to my colleagues in Bakırköy Ruh Sağlığı ve Sinir Hastalıkları Hastanesi and our department chief because of their understanding and support. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10025t2.jpg] [gm10025t3.jpg] [gm10025t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}