 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
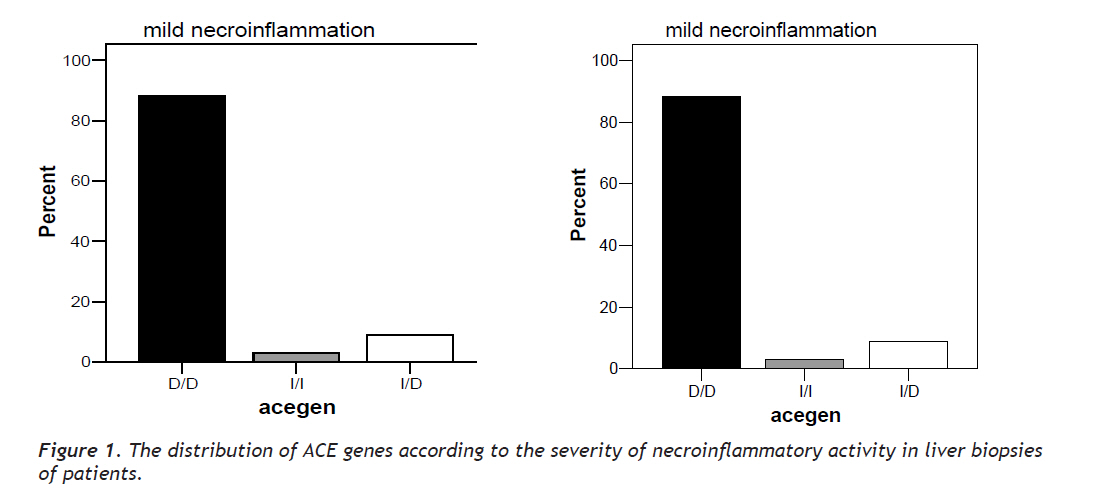
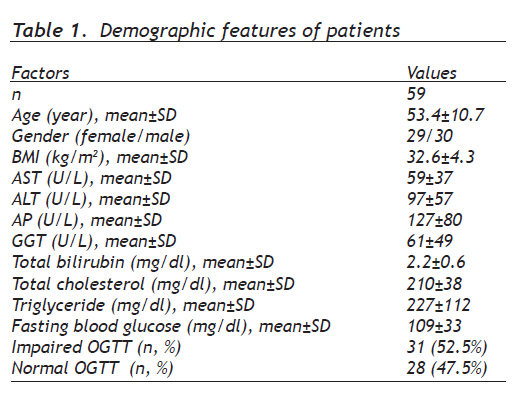
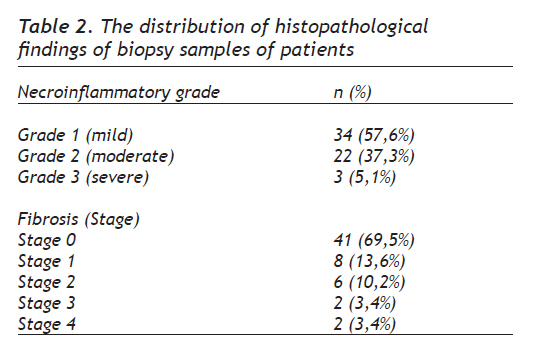
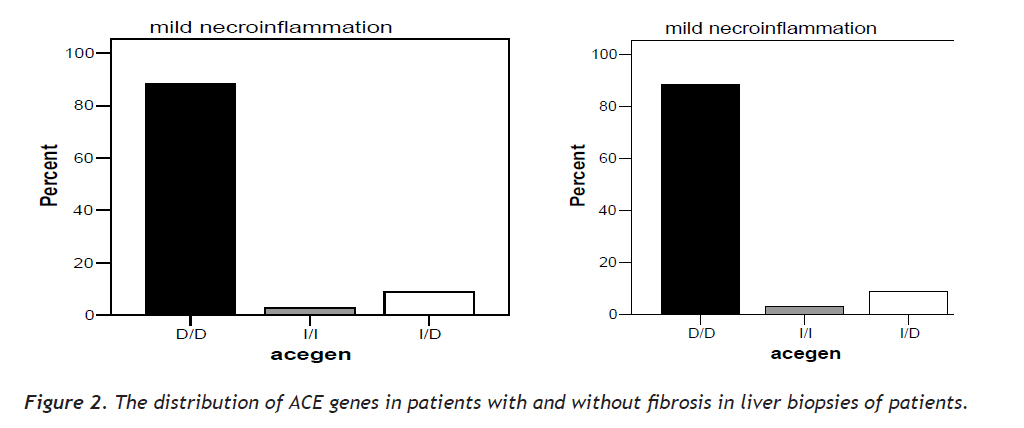
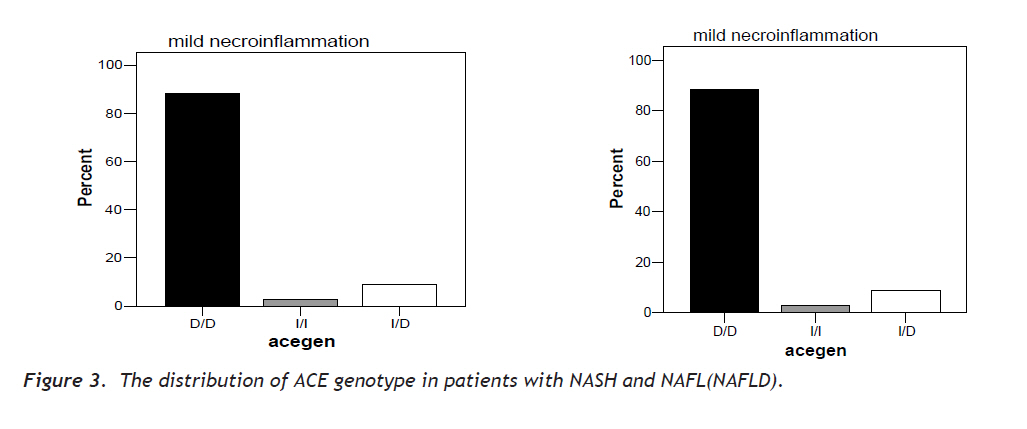
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 136-142 Original Article Angiotensin Converting Enzyme Gene (I/D) Polymorphism and Nonalcoholic Fatty Liver Disease Anjiotensin Gen(I/D) Polimorfizmi Ve Nonalkolik Yağlı Karaciğer Hastalığı Mustafa Güçlü, Tolga Yakar , Ender Serin Başkent University, Faculty of Medicine Adana Application and Research Hospital, Gastroenterology Clinics, Adana, Turkey Correspondence: Dr.Mustafa Güçlü, Mustafa GÜÇLÜ, Department of Gastroenterology, Maremar Medical Center Şehit. Ab. Çav. Alp. Tur. Bul. Nev. Ongun Sit. no: 41, K: 5/10, K.Maraş/ Turkey, Phone: 90 344 225 95 95, Fax: 90 344-2217378, E-mail: mgbaskent@hotmail.com Received: 04.04.2009 Accepted: 27.08.2009 Code Number: gm10027 ABSTRACT Aim: Fibrosis is a finding showing that the process can be progressive in the spectrum of non-alcoholic fatty liver disease. Activated hepatic stellate cells cause fibrosis induced by angiotensin II. In this study the relation between ACE gene (I/D) polymorphism and steatosis, necroinflammation and fibrosis in liver were investigated. Key words: Nonalcoholic fatty liver disease, ACE gene, hepatic steatosis Amaç: Nonalkolik yağlı karaciğer hastalığı (NAYKH) fibrozis ile sonuçlanan ve siroza kadar ilerleyebilen klinik bir antitedir. Aktive olmuş hepatik stellat hücreler, anjiotensin II (AT-II) tarafından indüklenerek fibrozise yol açmaktadır. Bu çalışmada ACE geni (I/D) polimorfizmi ile karaciğerde steatoz ve fibrozis arasındaki olası ilişkiler araştırılmıştır. Anahtar kelimeler: Nonalkolik yağlı karaciğer hastalığı, ACE gen, hepatik steatozis INTRODUCTION Nonalcoholic fatty liver disease (NAFLD) includes a spectrum of hepatic pathology consisting of simple steatosis (type 1), steatosis plus lotbular inflammation (type 2), steatosis plus balloning degeneration (type 3), and steatosis plus balloning degeneration plus Mallory bodies or fibrosis (type 4) (1). Nonalcoholic steatohepatitis (NASH) represents type 3 and 4 histologic changes and is considered to be a progressive form of this entity (1). NAFLD is commonly seen in conjunction with features of the metabolic or insulin resistance syndrome, which include obesity, hypertension, diabetes mellitus, hyperlipidemia and hypercholesterolemia. Metabolites and cytokines formed during lipid peroxidation, which is accepted in NASH pathogenesis cause increase in collagen synthesis and fibrosis by activating hepatic stellate cells (HSC) (2). The renin-angiotensin system (RAS) has been said to be involved in the pathogenesis of several diseases including fibrosis in the liver, kidney, heart and lung during chronic inflammation through the regulation of cell growth, inflammation, oxidative stress and fibrosis (3). The key enzyme in this system is the angiotensin converting enzyme (ACE) which converts angiotensin-I (AT-I) to the potent vasoconstrictor angiotensin-II (AT-II). ACE gene localized in 17th chromosome is composed of 26 exons (4). A polymorphism as the presence (insertion, I) or absence (deletion, D) of a 300 base pair in Alu repeat site localized in 16th intron of human ACE gene. The ACE-D, a deletion polymorphism of a 287-bp fragment of intron 16 of the ACE gene allele, has been shown to result in higher levels of circulating enzyme in a dose dependent manner (4). The role of the ACE gene I/D polymorphism as a risk factor has been investigated in several diseases (5). There are two types of angiotensin receptors; AT-I and AT-II receptors. AT-II exerts its known pharmacological effects via AT-I receptor. AT-II, exerts its effects via receptors on cell surface. The findings that angiotensin converting enzyme inhibitors (ACE-I) and AT-II receptor antagonists decrease hepatic fibrosis support the effects of angiotensin and its receptors on liver fibrosis (6). It was found that serum ACE levels were found to be increased approximately two times in people with DD allele of ACE gene and also it was reported that increased serum angiotensin II levels in people with DD allele were associated with insulin resistance, systemic hypertension, atherosclerosis, coronary artery disease and diabetic nephropathy (7). In our study we aimed to investigate the role of polymorphism of ACE gene in NAFLD pathogenesis. MATERIALS AND METHODS Patients The present study was initiated after an approval from the Ethical Committee of Baskent University Faculty of Medicine. For the study inclusion and liver biopsy signed informed consent was taken from each patient. We defined non-alcohol use as 30 g/day or less for men and 20 g/day or less for women. Exclusion criteria were positive viral markers (such as hepatitis B and C), history of alcohol use, diagnosis of autoimmune hepatitis, liver disease associated with drug use, primary biliary cirrhosis, metabolic liver diseases (such as hemochromatosis and Wilson disease). No patient had conditions related to secondary NAFLD such as regular use of drugs known to produce steatosis (corticosteroids, tamoxifen, amiodarone), previous gastrointestinal surgery, total parenteral nutrition. Ultrasonography (USG) is extensively preferred in NAFLD/NASH diagnosis and shiny liver is observed due to the increase in echo. While the sensitivity and specificity of USG are 89-95% and 84-93% respectively; they are 57-77% and 85-89% in the presence of liver fibrosis (8). Additionally; oral glucose tolerance test (OGTT), aspartat aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (AP), gamma glutamyl transferase (GGT), total billirubin and fasting blood glucose (FBG) were measured. Methods NAFLD was diagnosed histologically. All liver biopsy samples were obtained by percutaneous route using tru-cut biopsy needle. Formalin-fixed, paraffin-embedded liver sections were stained routinely with hematoxylin and eosin, silver reticulin, Masson trichrome, Perls’ Prussian blue, and diastase-resistant periodic acid-Schiff. Fatty change was defined as 10% or more fatty metamorphosis in the hepatocytes. Patients demonstrating only steatosis and lobular inflammation in their biopsy results were not considered to have NASH and this group of patients was named as NAFLD. Either ballooning degeneration of hepatocytes, Mallory bodies and/or fibrosis had to be present to confirm the diagnosis of NASH. Studies on the liver specimens included a semiquantitative assessment of the grades of steatosis (mild or grade 1, 10%-33% of hepatocytes affected; moderate or grade 2, 34%-66% of hepatocytes affected; severe or grade 3, >66% of hepatocytes affected); of inflammatory activity (according to Brunt classification) and of fibrosis (according to Brunt classification) (9). Brunt classification of fibrosis assessment includes five stages: stage 0, no fibrosis; stage 1, zone 3 perisinusoidal or pericellular fibrosis, focally or extensively present; stage 2, zone 3 perisinusoidal or pericellular fibrosis with focal or extensive periportal fibrosis; stage 3, zone 3 perisinusoidal or pericellular fibrosis and portal fibrosis with focal or extensive bridging fibrosis; stage 4, cirrhosis. ACE GENE I/D Genotyping: Genomic DNA to be used in molecular analysis was isolated by salt precipitation method from 10 ml of peripheral blood sample drawn from individuals in the study. The analysis of I/D polymorphism that is located in 16th intron of ACE gene, was performed with Polymerase Chain Reaction (PCR). For each PCR reaction the reaction mix prepared as the end volume to be 25l by using 10 pmol/uL F 5’CTGGAGACCACTCCCATCCTTTCT3’ and R5’GATGTGGCCATCACATTCGTCAGAT3’ primers, contained 4 dNTP (Roche-Almanya), 10XPCR tamponade (100mM Tris-HCl, 15 mM MgCl2 , 500mM KCl, pH : 8.3) (Roche-Almanya), 1.25U Taq DNA Polymerase and 100 ng genomic DNA with a concentration of 30mol/l. Reaction was performed in 35 cycles each composed of denaturation in 95 OC for 5 minutes, annealing in 94 OC for 30 seconds and extension in 69OC for 45 seconds. After DNA amplification, PCR products were taken on 2% agarose gel electrophoresis and consequently analysed under UV light by staining etidium bromide. A band of 190 bp shows deletion (D) and a band of 490 bp shows insertion (I). Statistical analysis The data were analyzed and compared by the Student t test and χ2 test coefficient in SPSS software ver.11. P values of <0.05 were considered statistically significant. RESULTS The demographic characteristics and clinical measurements showed in Table 1. In patients mean body mass index (BMI) was 32,65±4,34 kg/m2 mean triglyceride was 227,59±112,89 and total cholesterol was 210,53±38,99 mg/dl. In patients normal and impaired OGTT was present in 28 (47,5%) and 31 (52,5%) patients respectively. When ACE gene was compared by means of I/D genotypes, D/D genotype was observed in 86,4% (in 51 of 59 patients) in patients. I/D genotype was determined in 5,1% (3/59) of patients. While I/I genotype was determined in 8,5% (5/59) in patients. In liver biopsies of the patient while fibrosis of 0, 1, 2, 3, 4 according to Brunt classification histopathologically were present in 41, 8, 6, 2 and 2 patients respectively, there were 34, 22 and 3 patients with grade 1 (mild), grade 2 (moderate) and grade 3 (severe) necroinflammatory activity respectively (Table 2). There was no significant association between ACE gene (I/D) polymorphism and necroinflammatory activity and fibrosis (p>0.05) (Figure 2,3). Histopathologically 55.9% (33/59) of the patients suffered from NASH and 44.1% (26/59) from simple steatosis. There was no significant association with ACE gene (I/D) polymorphism between both groups (p>0.05). While 88.5% (23/26), 7.7% (2/26) and 3.8% (1/26) of NAFLD patients had D/D, I/I and I/D genotype frequency respectively; out of patients with NASH 84.8% (28/33) had genotype D/D, 3% (1/33) had I/I, 12.1% (4/33) had I/D and there was no statistically significant relation between both groups by means of genotype frequency (Figure 3). In patients, 31 patients (52.5%) with impaired OGTT were determined. The distribution of DD, ID, II genotypes of ACE gene in patients with impaired and normal OGTT were 26 (%51) versus 25 (49%) (p>0.05), 2 (66,7%) versus 1 (33,3%) (p>0.05) and 3 (60%) versus 2 (40%) (p>0.05) respectively. While there was no significant association between impaired OGTT and necroinflammatory activity in liver biopsy in NAFLD group, a significant relation was determined with fibrosis (p<0.05). DISCUSSION NAFLD is a pathology, which can cause cirrhosis, end stage liver insufficiency and hepatocellular carcinoma, which can require liver transplantation and result in liver based death. Thus, the identification and knowledge of factors causing the progression of the disease are important. Major risk factors for NAFLD are diabetes, hyperlipidemia and obesity. On the other hand NAFLD is considered as a feature of metabolic syndrome X or insulin resistance syndrome (IRS) (10). Oxidative stress formed as a result of fatty liver is a major and critical risk factor for HSC activation. HSC activation induces liver fibrosis (11). The RAS has been said to be involved in the pathogenesis of several diseases including fibrosis in the liver, kidney, heart and lung during chronic inflammation through the regulation of cell growth, inflammation, oxidative stress and fibrosis (12). The key enzyme in RAS is ACE and is coded by ACE gene. It has been reported that DD allele of ACE gene is associated with increased serum levels of angiotensin II, insulin resistance, systemic hypertension, atherosclerosis, presence of coronary artery disease, and progression of diabetic nephropathy (13). The ACE plays a central role in this system by converting angiotensin I to the potent vasoconstrictor angiotensin II. Angiotensin II stimulates the proliferation of hepatic stellate cells, cardiac fibroblasts, and mesangial cells and increases the synthesis of extracellular matrix proteins(14,15). The deletion type polymorphism in the 16th exon of the ACE DD genotype is associated with elevated serum and cellular ACE levels. This genotype is associated with several disorders including cardiac and renal diseases (5). However, the pathological risk of ACE DD genotypes also varies between populations with different genetic and environmental backgrounds, suggesting that the ACE DD genotype is acting as a disease modifier rather than as a disease susceptibility factor (16). In our present study no significant association was determined between DD, DI and II genotype frequency of ACE gene and fibrosis in liver histology. These findings show that there was a positive association between the increase in the frequency of D allele of ACE gene and liver steatosis while a negative association was observed between decrease in I allele frequency. On the other hand when patients were evaluated as NASH and NAFLD histopathology, no significant association was determined between both groups by means of the distribution of genotype frequency of ACE gene. These findings show that results we obtained such as the high frequency of DD genotype of ACE gene in insulin resistance, systemic hypertension, diabetes and coronary heart disease which can be members of metabolic syndrome in NAFLD/NASH group, reflection of metabolic syndrome. Impaired OGTT is a part of IRS. The relation between IRS and TNF-α is known. TNF-α, NF-Κβ and Transforming Growth Factor β (TGF-β) cause a progression of fibrosis by stimulating HSC proliferation. However; while there was no association between impaires OGTT and necroinflammatory grade in liver histology, a significant relation was determined with liver fibrosis in our study. Although insulin resistance was not evaluated in this study, the association between the level of insulin resistance and fibrosis is known and there is a relation between OGTT and IR (17,18). Systemic infusion of AT-II results in significant cardiac and renal fibrosis (19). Interestingly a fibrogenic response can’t be determined in liver. All these findings show that AT-II increased liver fibrosis through HSC, which is activated in damaged liver and a target for AT-II by expressing AT -I receptors in cell surface, while AT-II had no effect on normal healthy liver. In our study the frequency of DD genotype to be higher in individuals with fatty liver and thus causing higher levels of serum AT-II levels however we didn’t measured but no association with necroinflammation or the level of fibrosis suggest that high frequency of AT-II related with DD genotype prepared a background for disease progression in association with fattening which is the first move and that it is not responsible from direct progression. There are currently no specific treatments for NASH. Therapy is empirical focusing on conditions such as obesity, insulin resistance, diabetes and dyslipidaemia. Better knowledge of the molecular mechanisms associated with insulin resistance and activation of hepatic stellate cells may provide effective targeted therapy. It was found that serum ACE levels were increased in individuals with DD allele of ACE gene and also in individuals with DD allele increased serum angiotensin II levels were associated with insulin resistance, systemic hypertension, atherosclerosis, coronary artery disease and diabetic nephropathy (14). On the other hand there are publications reporting that the efficacy of ACE-I/ATRA treatment didn’t interact with ACE gene (20). The relations between ACE genotypes and disease progressions and interactions of ACE-I/ATRA treatments with these genotypes and the pathological and biochemical interactions are not yet completely known. Due to the finding that ACE DD genotype was significantly high in NAFLD patient group and that this genotype was associated with serum ACE activity and increased levels of AT-II, it can be expected that ACE-I/ATRA treatment in hepatic inflammation would regress hepatic inflammation and fibrosis. In summary our results show that frequency of D/D genotype was higher in NAFLD/NASH patient group but it didn’t have any effect on necroinflammatory activity and fibrosis. However the predominance of D/D genotype in NAFLD/NASH patient group might be a reflection of metabolic syndrome. In this case it seems as ACE DD genotype plays a role in the development of steatosis, which is known as the first move of NASH pathogenesis. In studies performed with ACE-I / ATRA which have been recently used in hepatology. The association of the I/D polymorphism of ACE gene with response to treatment and disease progression has not been investigated. However it is clear that such associations will be investigated in the future. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10027t1.jpg] [gm10027f3.jpg] [gm10027f1.jpg] [gm10027f2.jpg] [gm10027t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}