 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
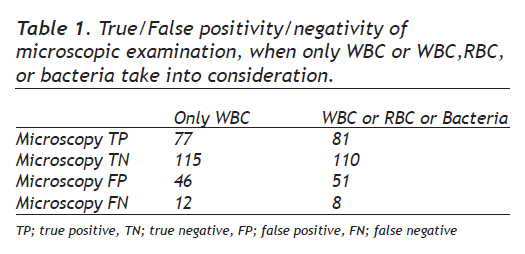
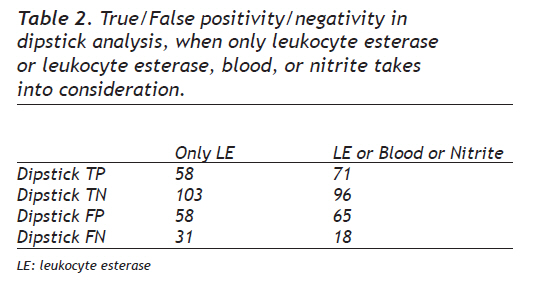
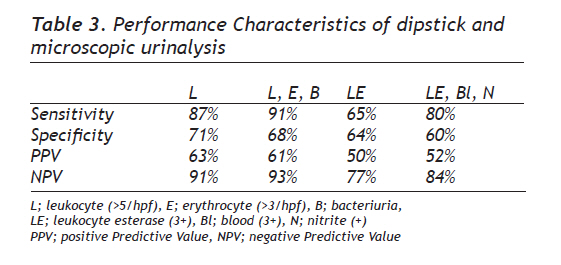
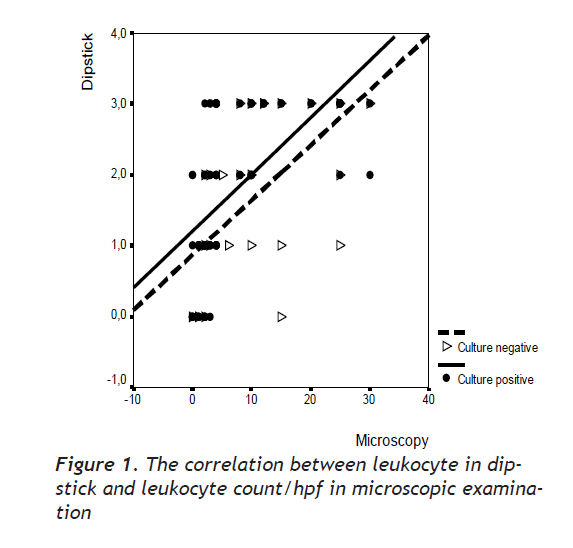
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 174-178 Original Article Performance Characteristics of Dipstick and Microscopic Urinalysis for Diagnosis of Urinary Tract Infection İdrar yolu enfeksiyonu tanısında striple ve mikroskopik idrar analizinin performans özellikleri Ramazan Memişoğulları, Hatice Yüksel, Hayriye Ak Yıldırım, Özlem Yavuz Düzce University, School of Medicine, Department of Biochemistry, Düzce, Turkey Received: 12.06.2009 Accepted: 15.09.2009 Correspondence: Ramazan Memişoğulları, Department Of Biochemistry, Düzce University, School Of Medicine, 81620 Düzce, Turkey Fax: +903805421387 Phone: +903805421386 E-mail: rmemisogullari@hotmail.com Code Number: gm10029 ABSTRACT Aim: Although the urine culture is used as the reference standard to determine presence or absence of urinary tract infection, the culture is an expensive and time-consuming method. The objectives of the study were to compare dipstick urinalysis with microscopic urinalysis and to compare dipstick and microscopic urinalysis results with urine culture results, by calculating performance characteristics of these tests. Key words: Dipstick, urine microscopy, urine culture, sensitivity, specificity, predictive values Amaç: İdrar kültürü idrar yolu enfeksiyonunun saptanmasında referans test olarak kabul edilmekle beraber pahalı ve zaman gerektiren bir testtir. Çalışmamızın amacı, striple idrar analizi ve mikroskopik idrar analizini karşılaştırmak, strip ve mikrosopik idrar analizi sonuçları ile idrar kültür sonuçları arasındaki ilişkiyi bu testlerin performans özelliklerini ölçerek değerlendirmektir. Anahtar kelimeler: Strip, idrar mikroskopisi, idrar kültür, sensitive, spesifite, prediktif değer INTRODUCTION Urine samples constitute a major proportion of the samples tested in routine diagnostic laboratories. Although the urine culture is used as the reference standard to determine presence or absence of urinary tract infection, the culture is an expensive and time-consuming method (1). Substituting a urine dipstick test or urine microscopy for a hospital laboratory urinalysis may be less time-consuming and less expensive, but also some doubts are present about that the urinalysis may not be as accurate. There are still different opinions regarding whether urinalysis or urine culture should be a routine. A complete consensus whether culture should be performed only for specific indications has yet not concluded. The objectives of the study were; 1) to compare dipstick urinalysis with microscopic urinalysis, 2) to compare dipstick and microscopic urinalysis results with urine culture results, by calculating performance characteristics of these tests. MATERIALS AND METHODS Collection of the Specimens The 250 freshly morning urine specimens, collected under sterile conditions as far as possible were studied. All samples were completely processed within 1–2 h after arrival, to avoid overgrowth of any contaminating bacteria. Patients who had taken antibiotics in the past 72 hours, or had indwelling Foley catheters, symptomatic vaginal discharge, diabetes mellitus, or immunodeficiency disorders were excluded. Specimens containing squamous epithelial cells were not excluded from analysis because other investigators have found that the presence of squamous cells does not affect the diagnostic accuracy of the test (2,3). Urine samples were divided into 3 sterile aliquots, 2 for urinalysis and 1 for urine culture. Urine Dipstick Chemical Analysis A complete urinalysis included physical, chemical, and microscopic examinations. Combur 10-Test M strips on a Miditron-M semi-automated reflectance photometer (Roche Diagnostics GmbH, Mannheim, Germany) have been used in our routine laboratory for chemical examinations. Our laboratory technician was skilled in the dipstick procedure. The technician tested the first aliquot immediately using Combur 10 Test M reagent strip (Roche Diagnostics GmbH, Mannheim, Germany) for urinalysis from a sealed, air-tight container that had been opened within the past 10 days. The strips include reagent pads for semiquantitative assessment of nitrite, leukocyte esterase, pH, specific gravity, protein, glucose, ketones, urobilinogen, bilirubin, and blood. The leukocyte esterase measurement was read after 2 minutes and recorded as negative, trace, small (1+), moderate (2+), or large (3+). The nitrite measurement was read at 60 seconds and recorded as negative or positive. The blood measurement was also read at 60 seconds and recorded as negative; (1+), (2+), (3+), (4+). Cutoff values for a positive result was (3+) leukocyte esterase, or (3+) blood, or nitrite (+). Day-to-day imprecision was assessed with control material: Liquichek Urinalysis Control Levels 1 and 2 (Bio-Rad). This is stable for 30 days when stored tightly capped at 2–8 °C. Microscopic Urinalysis A 10-mL aliquot of urine was centrifuged at 1500 rpm for 5 minutes. The supernatant was removed and the sediment was resuspended into solution with 1 mL of supernatant. One drop (0.4 mL) of the resuspended sediment was placed onto a microscope slide, covered, and examined under ×100 and ×400 magnifications. The results as the number of WBCs and RBCs per high-power field (hpf) and bacteriuria (×400 magnification) were interpreted. Cutoff values for a positive result was more than 5 WBCs/hpf or more than 3 RBCs/hpf or bacteriuria. Urine Culture Of the total of 250 urine samples examined, 89 gave a pure growth of 105 or more organisms per ml (‘culture positive’ samples). The remaining 161 samples were reported as ‘culture negative’ samples. If 3 or more distinct species of bacteria were present in culture and were not considered uropathogens, the culture was considered contaminated and classified as negative (9 samples). Calculation of sensitivity, specificity, and predictive values Sensitivity, specificity, and predictive values were calculated for leukocyte esterase, nitrite, or blood on dipstick and for RBCs, WBCs, or bacteria on microscopic urinalyses. Sensitivity, specificity, and predictive values were calculated as follows (4): Sensitivity=True positive/(True positive+False negative) Specificity=True negative/(True negative+False positive) Positive Predictive Value= True positive/(True positive + False positive) Negative Predictive Value= True negative/ (True negative + False negative) Statistical Analysis Pearson’s correlation test was used to evaluate the correlation between leukocyte in dipstick and leukocyte count/hpf in microscopic examination RESULTS Thirty-five point six percent (89/250) of patients had urine cultures with 105 colonies/mL or greater. The main organisms grown from the culture positive cases were Escherichia coli (61), Klebsiella (14), Citrobacter (2), Pseudomonas (3), Enterobacter (5), and Staphylococcus (4). Nine cultures were considered contaminated and classified as negative. Performance Characteristics Table 1, 2, and 3 shows performance characteristics of microscopic or dipstick urinalysis. When at least one of the leukocytes esterase, nitrite, or blood in dipstick; one of the leukocyte, erythrocyte, or bacteria in microscopic examination was taken into consideration, sensitivity and specificity of microscopic urinalysis were 91% and 68%, and of dipstick urinalysis were 80% and 60%, respectively. Negative predictive values were 84% for urine dipsticks and 93% for microscopic urinalysis. Positive predictive values were 52% and 61% for dipstick and microscopic urinalysis, respectively. Correlation of leukocyte analyses between microcopy and dipstick A strong correlation was present between leukocyte esterase and microscopic leukocyte count/hpf both in culture negative group (r=0.57; p<0.001) and in culture positive group (r=0.75; p<0.001) (Figure 1). DISCUSSION In the present study, dipstick and microscopic urinalysis results were compared with urine culture results, which were used as the reference standard to determine presence or absence of urinary tract infection. The present study demonstrates that bedside urine dipsticks and microscopic urinalysis may be substituted for rapid urinalysis to diagnose uncomplicated urinary tract infections. Use of dipsticks and microscopic urinalysis instead of urine culture may decrease patient time and the cost of testing. Urine culture has the disadvantage of taking at least 48 hours to give a result. More rapid methods of urinary tract infection diagnosis are therefore desirable. The most widely used rapid tests are dipsticks. Dipstick tests have the advantage of being quick and easy to perform and can be carried out in primary care giving an immediate result. Microscopic examination of urine samples for leukocytes, erythrocytes or bacteria is considerably more time consuming and labor intensive than the dipstick method (5). But false positive and false-negative rates are significantly higher as compared with the microscopic examination. In dipstick analysis, urinary protein excretions in excess of 500 mg/dL and urinary glucose excretions in excess of 2 mg/dL may diminish the intensity of the reaction color, as can cephalexin and gentamicin if administered in high daily doses, or boric acid if used as a preservative. The nitrite test depends on the conversion of nitrates into nitrites by bacteria in the bladder. It requires an incubation period of several hours in the bladder and so is best performed using an early morning urine sample. In the study, all specimens were morning urine samples. Unfortunately some organisms, especially gram-positive ones, do not convert nitrates into nitrites. Previous evaluations of the predictive value of combining leucocyte-esterase and nitrite tests have produced conflicting results (6-8), but the present study suggests these tests to be of value. In the present study, when only leukocyte esterase takes into consideration, sensitivity and specificity was 65% and 64%, respectively, whereas sensitivity and specificity in microscopic examination, when only leukocyte esterase takes into consideration, was 87% and 71%, respectively. When leukocyte esterase, or blood, or nitrite takes into consideration, sensitivity increased to 80% from 65%, however specificity decreased to 60% from 64% due to increased false positives. In the same way, when WBC, or RBC, or bacteria take into consideration, sensitivity increased to 91% from 87%, however specificity decreased to 68% from 71% due to increased false positives. In the present study, when divided into 2 groups as culture positive and negative, a strong correlation between leukocyte esterase and microscopic leukocyte count/hpf was present both in culture positive group and in culture negative group. Rapid diagnosis or exclusion of urinary tract infection is valuable both to the general practitioner and to the hospital physician. Therefore, dipstick test may be performed when a very rapid conclusion was desired. Microscopy of the urine is recommended in textbooks for the diagnosis of urinary tract infections (9). However, it is reported that less than a third of general practitioners had a microscope; this instrument also appears to be rarely found on the modern hospital wards (10,11). In the study, accuracy of microscopic examination was higher than those of dipstick test. Cutoff values for a positive result was more than 5 WBCs/hpf or more than 3 RBCs/hpf or bacteriuria. The study has suggested that both urinalysis methods may be used for rapid diagnosis. Therefore, because urine culture is an expensive test, nitrite, leukocyte, or blood test in dipstick or leukocyte, erythrocyte, or bacteria in microscopic examination may be guiding analytes before culture. Acknowledgments The authors thank Biolog Erdoğan ŞAHİN and Assoc. Prof. Dr. Tevfik YAVUZ, working in Training and Research Hospital of Düzce University, Biochemistry and Microbiology Laboratory, respectively, for their technical assistances. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10029t3.jpg] [gm10029t1.jpg] [gm10029f1.jpg] [gm10029t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}