 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
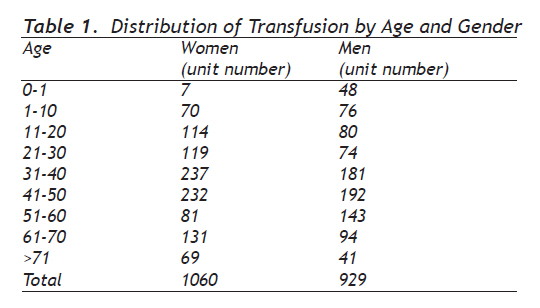
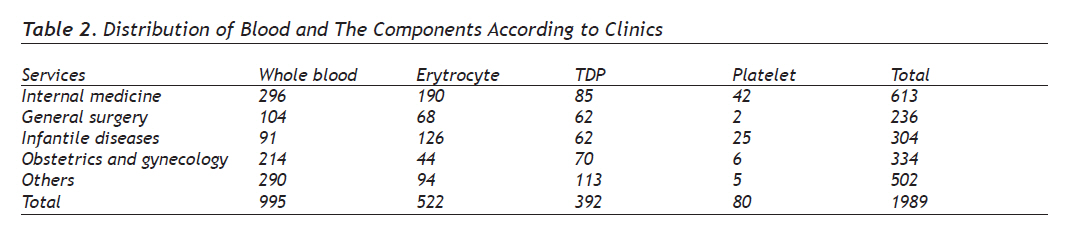
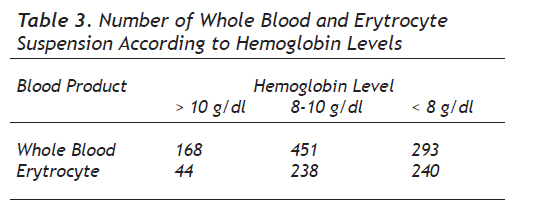
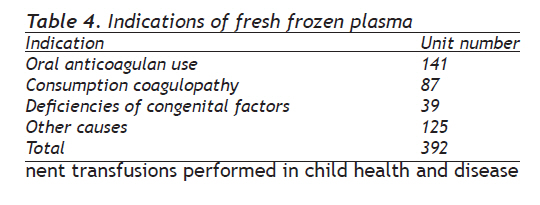
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 143-149 Original Article Distribution of Blood and Blood Components, Indications and Early Complications of Transfusion Kan ve Kan Bileşenlerinin Dağılımı, Transfüzyonun Endikasyonu ve Erken Komplikasyonları Servet Efe, Cengiz Demir, İmdat Dilek Yüzüncü Yıl University, Medical Faculty, Department of Internal Medicine, Division of Hematology Correspondence: Cengiz Demir, Yuzuncu Yıl University, Medical Faculty, Department of Internal Medicine, Division of Hematology 65200 Van, Turkey Tel: 90 432 2164706 Email: drcengizdemir@hotmail.com Received: 24.06.2009 Accepted: 27.10.2009 Code Number: gm10030 ABSTRACT Aim: It is aimed in this study to determine blood and blood component’s transfusion indications, component using rate, early transfusion complications and the distribution of complications according to the blood component. Key words: Blood, transfusion, early complication, indication, component Amaç: Bu çalışma, kan veya kan komponentinin, transfüzyon endikasyonları, komponent kullanma oranları, erken dönem transfüzyon komplikasyonları ve komplikasyonların verilen kan komponentine göre dağılımını belirlemek amacıyla yapılmıştır. Anahtar sözcükler: Kan, transfüzyon, erken komplikasyon, endikasyon, bileşen INTRODUCTION The purpose of a blood transfusion is to replace lost blood, to increase the flow rate of cardiac, to increase blood elements, to replace the missing clotting factors and immune system elements. Blood and blood component transfusion is a serious event. Therefore, blood or components transfusion must be made within the appropriate indication after careful evaluation of clinical status. Benefit-risk assessment must be made each time (1). The serious complications of transfusion that can lead to damage should always keep in mind (2). Complications related to blood transfusion may be considered under three main headings including hemolytic reactions, nonhemolitik reactions and infectious complications (3). Hemolytic, allergic, febrile nonhemolitic transfusion reactions (FNHR), fluid loading, transfusion-related lung damage, anaphylactic and metabolic reactions are main acute reactions and they can be seen within the first 24 hours after transfusion (4). Patient’s follow-up doctor has primary responsibility for transfusion of blood and health team should also have information about the complications which can be seen after transfusion. Transfusion-related complication may develop in different rates and violence depend on associated with different situations including blood or component availability, the genus, given the speed, the recipient’s disease state and the findings in the disease. Rate of transfusion-dependent complications can vary according to medical facilities. FNHR have been reported as the most common transfusion-related complications (5). Transfusion indications, utilization rates and rates of blood and component use and complications of transfusion data do not have sufficient extent in our country. Also, there is no data associated with these events in our region. Therefore, this study has been planned to determine 1989 units of blood and blood component’s transfusion indications, component using rate, early transfusion complications and the distribution of complications according to the blood component which is taken from Yuzuncu Yıl University Medical Faculty Hospital’s blood center for transfusion. MATERIALS AND METHODS In this study, blood and blood component (which transfer from Yuzuncu Yıl University Medical Faculty Hospital to clinic for transfusion of 1010 patients) use was assessed. Transfusions indications of received blood and blood products, the component using rates, complications of early transfusion, distribution of complications according to received blood component has been prospectively investigated in this study. In this study, recipient’s name, surname, age, gender, barcode number, blood component, blood group, the clinic where transfusion have done, transfusion indications, whether or not transfusion history, the amount and type of blood component, previous blood transfusion complication and type, product waiting period in the blood center, amount of volume and elapsed time until the development of reaction, vital findings before and after transfusion (blood pressure, pulse, fever and breathing number) were recorded during use of blood and blood component. When blood was requested the clinic the patient’s blood centrifuged for 5 min at 5000 rpm and then test by forward and reverse tube method to determine his or her blood group. Then determination of eligibility is made by the cross-comparison for full blood and erythrocyte suspension. Previously prepared forms were submitted to clinic with component. The patient’s arterial blood pressure, heart rate, number of respiratory, fever, and history of transfusion sent by responsible physician has been saved the form. In the same way, vital findings after the transfusion were recorded in the relevant sections of the form. Developing reactions within 24 hours after the transfusion was regarded as acute transfusion reactions. When complication occurred, type and clinical feature of complication wrote in the relevant sections of the form. Then, forms received from the clinic and information has been saved to computer. When work was completed, all findings were statistically evaluated in the Excel work environment. RESULTS Number of units of blood and blood products transfused to patients (1010 patients; 566 women, 444 men) was 1989 (1060 units (53%) in women, 926 units (46.7%) in men). Average 1.96 units blood and blood products per patient were transfused (1.87 units in women; 2.09 units in men). Number of units of transfused whole blood, erythrocyte suspension and fresh frozen plasma (FFP) were 995 (50%), 552 (26%) and 392 (29.8%), respectively. Distribution of patients according to age and gender has been given in Table 1. The distribution of age of whole blood units transfused was as follows: 546 units fresh blood (54.9%), 269 (27%) units 2-5 days and 180 units (18.1%) >5 days. The distribution of age of erytrocyte suspension units transfused was as follows: 184 units fresh blood (35.2%), 181 (34.7%) units 2-5 days and 157 (30.1%) units >5 days. 613 units (30.8%) blood and blood component transfusions performed in internal medicine; 296 (48.2%) units were whole blood, 190 (31%) units were erytrocyte suspension 85 (13.8%) units were FFP and 42 (6.9%) units platelet suspension. 236 units (11.9%) blood and blood component transfusions performed in general surgery; 104 (44.1%) units were whole blood, 68 (28.8%) units were erytrocyte suspension 62 (26.3%) units were FFP and 2 (0.8%) units platelet suspension. 334 units (16.8%) blood and blood component transfusions performed in obstetrics and gynecology; 214 (64.1%) units were whole blood, 44 (13.2%) units were erytrocyte suspension 20.9% (70 units) were FFP and 6 (1.8%) units platelet suspension. 304 units (15.3%) blood and blood component transfusions performed in child health and disease clinic; 91 (29.9%) units were whole blood, 126 (14.4%) units were erytrocyte suspension, 62 (20.4%) units were FFP and 25 (8.2%) units platelet suspension. 502 units (25.2%) blood and blood component transfusions performed in other services; 290 (57.8%) units were whole blood, 94 (18.7%) units were erytrocyte suspension 113 (25%) units were FFP and 5 (1%) units platelet suspension (Table 2). 168 units of total 995 whole blood transfusion was recieved to patients with hemoglobin of 10 g/dl or higher in all services. 114 units (16.9%) and 54 units (32.2%) of these transfusions respectively were given to surgical patients and patients with active bleeding. 451 units of whole blood transfusion was recieved to patients with hemoglobin of 8 g/dl;193 units (42.8%) were given to surgical patients, 189 units (41.9%) were given to patients with active bleeding and semptomatic patients, 69 units (15.3%) were given to patients who take chemotherapy. 293 units of whole blood transfusion was recieved to patients with hemoglobin of <8 g/dl; 62 units (21.2%) were given to surgical patients, 165 units (41.9%) were given to patients with active bleeding and semptomatic patients, 66 units (22.5%) were given to patients who take chemotherapy. 44 units (%8.4) of total 552 erytrocyte suspension were recieved to surgery patients and patients with hemoglobin of 10 g/dl or higher. 238 units of erytrocyte suspension were recieved to patients with hemoglobin of 8-10 g/dl; 169 units (71.0%) were given to patients with active bleeding and semptomatic patients, 38 units (15.9%) were given to surgical patients, 31 units (13%) were given to patients who take chemotherapy. 240 units of erytrocyte suspension were recieved to patients with hemoglobin of <8 g/dl; 155 units (64.6%) were given to patients with active bleeding and semptomatic patients, 49 units (20.4%) were given to surgical patients and 36 units (15%) were given to patients who take chemotherapy (Table 3). 141 units (8.4%) of total 392 FFP were recieved to patients with active bleeding depens on coumadine use, 106 units (27%) were given to patients with INR of higher than normal levels and surgical patients, 39 units (9.9%) were given to patients with active bleeding depends on factor deficiency. 87 units (22.2%) were given to patients in intensive care unit depends on septicemia, disseminated intravascular coagulation vs, 13 units (3.3%) were given to patients underdoing biopsy with high level INR and 6 units (1.5%) were given to patients with higher levels INR because of organic phosphorus intoxification (Table 4). 45 units (8.4%) of total 80 units platelet suspension were recieved to patients with platelet levels below 10x109/L, 19 units (23.8%) were recieved patients with avarage platelet levels 10x109-30x109/L with bleeding, 13 units (16.2%) were recieved surgical patients with avarage platelet levels 30x109-50x109/L and 3 (3.8%) were recieved patients with platelet levels higher than 50x109/L. Transfusion related acute complication was observed in 3% (61) of patients; 1.8% (36) was FNHR. 1.9% of these complication were observed in patients recieved whole blood, [15.7% (3) fresh blood, 36.8% (7) 2-5 days blood and 47.3% (9) >5 days-old blood]. 2.3% of FNHR were observed in patients received erytrocyte suspension [33% (4) fresh, 16.6% (2) 2-5 days-old and 50% (6) >5 days-old erytrocyte suspension]. 6.25% of FNHR were observed in patients recieved platelet suspension. Distribution of FNHR percentage by transfusion number was as follow; 16.7% (6) were in first transfusion, 22.2% (8) were in second transfusion, 8.3% (3) were in third transfusion and 52.8% were in 5 and more transfusion. Urticaria was observed in 0.9% of cases (19). 0.9% of urticaria was developed in patients recieved whole blood (3; fresh blood and 6; >5 days-old blood). 1.1% of urticaria was related to erytrocyte suspension (3; fresh erytrocyte suspension and 3; >5 days erytrocyte suspension). Also 5% of urticaria was developed in patients recieved platelet suspension. Numbers of urticaria were 4 in first transfusion, 2 in second transfusions, 5 in third transfusions and 8 in 5 or more transfusion. Hypercalsemia was observed in one (0.5%) patients result of 6 units whole blood transfusion (4; >10 days-old blood, 2; fresh blood) (potassium level increased from 4.2 up to 6.1). Hypocalsemia was observed in two patients result of 5 and 10 units whole blood transfusion (calsium level decreased from 9.2 to 5.4 and from 8.3 to 5.8, respectively). Hypotension was observed in one patients after 2 units whole blood transfusion and in one patients after 1 unit erytrocyte suspension transfusion (120/80 - 90/60 and 150/80 - 90/65 mmHg, respectively). Also hypertansive attact was observed in one patients after 1 unit blood transfusion (120/70 - 210/130 mmHg). Distribution of acute transfusion reaction according to blood component has been given in Table 5. DISCUSSION Although full blood usage indications are limited, utilization rates are still high in transfusion medicine in our country. If bloods are used appropriately whole blood must be 3-5% of all products delivering from blood bank (6). 60.4% of the 187212 units blood was found to be whole blood and whole blood usage rate is reported to be 26.4%, 84.3%, 59.8%, and 78.9% in university hospitals, the Ministry of Health hospitals, Kızılay and other hospitals, respectively (7). In study performed in Uludag university distribution of blood utilization rate was determined. Result showed that utilization whole blood rate which was 92% in 1992 decline to 17% in 1999 (8). In study performed in Malatya region it was reported that utilization rate of whole blood, erytrocyte suspension, FFP and platelet suspension were 19.3%, 33.9%, 34.9% and 11.9%, respectively (9). In our study, percentage of transfused products by product type was as follows: 50% whole blood, 26% erytrocyte suspension, 19.8% FFP, 4.2% platelet suspension. Rao et al reported that percentage of transfusion was as follows: 53% erytrocyte suspension, 16% platelet suspension and 22% FFP (10). We have found different utilization rates of whole blood by service. These rates were as follows: 48.2% in internal medicine, 44% in general surgery, 64% in obstetrics and gynecology, 30 % in child health and disease clinic, 25.2% in other service. It has been seen that ratio of using whole blood is high and using platelet and fresh frozen plasma is low in our hospital. This situation has shown that whole blood using indications should determine more carefully. Indication for whole blood transfusion are patients with acute bleeding, trauma (large volume blood lose >25%) and surgical patients, cardiac surgery in infant and exchange transfusion. It is seen that there are very few indications for the use of whole blood transfusions and although the product has limited indication, it has a higher using rate and it’s showing that transfusion indications are not using for appropriate indications. Fernando et al reported that whole blood usage rate was 31.7%, 14.6%, 11.6% and 19.9% in intensive care units, surgery section, emergency service and internal section, respectively (11). We have seen that, rate of blood and blood component rate was 30.8%, 11.9%, 15.3% and %16.8 in internal diseases, general surgery, child health and disease, obstetrics and gynecology clinics, respectively. Rate of FNHR has been reported to be 0.1-2 (12,13). In study performed in Uludag University Medical Faculty Hospital reported that FNHR rate was 4.2 % (14). Ileri et al have done a study on children with acute leukemia and they reported that 3 (0.53%) FNHR, 4 (0.7%) urticaria and 3 (%0.5) platelet alloimmunizasion were observed during study (15). In our study transfusion related complications were observed in 3.1% (61) of patients. 1.8% (36) of complication was determined as FNHR. In another study it is reported that overall incidence of FNHR was found to be 0.09% result of transfusion of erytrocyte suspension (16). Again, rate of FNHR was found to be 2.15% in patients with erytrocyte suspension in another study (17). Also this rate was reported to be 1.1-12% in other two different studies, respectively (18,19). In our study erytrocyte suspension transfusion related FNHR rate was found to be 2.3%. Christian et al reported that FNHR was observed in 31 cases (0.09%) after 34867 platelet suspension transfusion (16). Anderson et al reported that FNHR were observed in 3% of patients with platelet suspension transfusion (20). This rate was reported to be 1.58% - 1.73% in other two studies, respectively (17,18). In our study FNHR was observed in 5 patients (6.25%) with platelet suspension transfusion. This rate has been seen low compared with studies above mentioned. Also some studies has been report higher rates. For example, Hedle et al have done a study on oncology patients with platelet suspension transfusion and they reported that FNHR rate was 20% (21). Also, Kelly et al determined the rate of FNHR to be 4.6 - 11.1% (22). In the study performed by Fernando et al, 2 (0.09%) FNHR was observed after 2028 FFP transfusion (11). Contarily, no FNHR was observed after FFP transfusion in our study. Developing allergic reactions during the transfusion occur against some substances found in donor plasma. In study performed in Uludag University Medical Faculty Hospital reported that 8 allergic reactions were detected after 312 blood transfusion units (14). Dzieczkowski et al reported that allergic reactions were detected at a rate of 51 per cent in patients with erytrocyte suspension transfusion (17). In the study performed by Sarkodee et al, allergic reaction rates reported to be 1.26% in patients with platelet suspension transfusion (23). Also, study performed by Hedle et al allergic reactions rates reported to be 4.8% (21). In our study uriticaria was observed in 19 patients (0.95%) and 9 (0.90%) of them was in whole blood transfused patients, 6 (1.14%) of them was in erytrocyte suspension transfused patients and 4 (5%) of them in platelet suspension transfused patients. It has seen that allergic reaction development rate is not different in literature. Hypotensive reactions to transfusion are less well recognized. In general, hypotensive reaction that occur administration of blood product through, a bedside leucoreduction filter in patients taking angiotensin-converting enzyme (ACE) inhibitors. The pathogenesis of these reactions involves bradykinin generation as blood is filtered over certain leucoreduction filters and ACE inhibitors prevent bradykinin breakdown (24,25). In the study that perform by Arslan et al, in one patient with chronic lymphocytic leukemia that was using cilazapril (ACE inhibitor) for hypertension, hypotension occured after given platelet suspension with leukocyte filter (26). Fried et al reported that observed hypotensive reaction following random donor platelet transfusion using beside white cell-reduction filter in a chronic lymphocytic leukemia patient who was treated with ACE inhibitor for her systemic hypotension (27). Also in our study, Hypotension was developed in one patients using ACE inhbitor after whole blood transfusion and one patient using ACE inhibitor after erytrocyte transfusion. Although the potassium level in the plasma increases during blood storage, this rarely causes hyperkalemia among recipients because potassium can be rapidly diluted, redistributed and excreted after the transfusion. However, a massive or rapid transfusion in a short period of time may cause hyperkalemia, particularly among premature infants and acidotic patients, and result in significant morbidities and even death (28,29). In our study, hyperkalemia was developed in only one patient after 6 blood transfusion units. Sodium citrate is the substance used to prevent blood coagulation during blood collection. When large volumes of blood are transfused, plasma citrate level increase and may develop hypocalcemia. In developed hypocalcemia result of high citrate; slower transfusion is sufficient. If patient have electrocardiogram changes and clinic findings, calcium gluconate is administered as a 10%. For replacement treatment, measurement of ionized calcium is preferred in patient with massive transfusion and liver disease (30). In our study, hypocalcemia was observed in patients after 5 blood transfusion units and in another patient after 10 units whole blood transfusion. As a result, findings obtained in our study; it has seen that whole blood utilization rates are high in our hospital. Information work should be increased to increase the use of component and to protect patients from unnecessary risk. The clinicians always should keep in mind that transfusion can lead to serious complication and benefit/risk assessment must take into account each transfusion. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10030t5.jpg] [gm10030t3.jpg] [gm10030t4.jpg] [gm10030t2.jpg] [gm10030t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}