 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
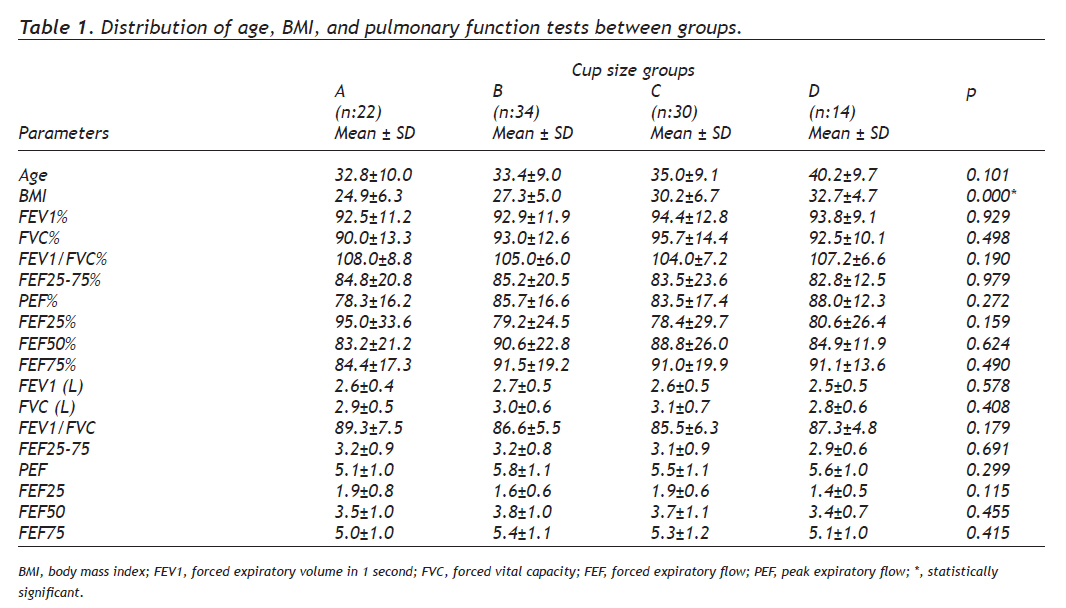
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 150-154 Original Article Effects of Breast Size on Lung Function Meme Boyutunun Solunum Fonksiyon Testleri Üzerine Etkisi Nurten Turhan-Haktanır1, Fatma Fidan2, Gülengül Köken3, Yavuz Demir1, Güray Yılmaz1, Şükrü İşler1, Murat Tüzüner1 Afyonkarahisar Kocatepe University, Faculty of Medicine, Departments of Plastic, Reconstructive, and Aesthetic Surgery1, Pulmonary Medicine2, and Obstetrics and Gynaecology3. Correspondence: Dr. Nurten Turhan-Haktanır, Afyon Kocatepe Universitesi, Plastik, Rek. ve Estetik Cerrahi AD, Afyonkarahisar, Türkiye. Fax: 90272 213 30 66, Phone: 90272 213 01 16 – 3012 E-mail: nurth70@yahoo.com Received: 17.04.2009 Accepted: 01.11.2009 Presented at 30th National Congress of Turkish Plastic, Reconstructive, and Aesthetic Surgery, October, 15-19, 2008, Antalya, Turkey Code Number: gm10031 ABSTRACT Aim: A few previous studies reported contradictory results about the effects of reduction mammaplasty on pulmonary function tests. This study was conducted to evaluate the effects of breast size on pulmonary functions in volunteer healthy adult women that, to the best of our knowledge, was not reported before. Key words: Breast; pulmonary function tests; body mass index Amaç: Redüksiyon mamoplastisinin solunum fonksiyon testleri üzerine etkisi konusunda birbiriyle çelişen sonuçlar daha önce bildirilmiştir. Çalışmamızda sağlıklı, gönüllü, yetişkin kadınlarda meme boyutunun solunum fonksiyon testleri üzerine etkisinin değerlendirilmesi amaçlanmıştır. Anahtar kelimeler: Meme; solunum fonksiyon testleri; vücut kütle endeksi INTRODUCTION Surgical reduction of large breasts has been increasingly performed not only for aesthetic complaints, but also physical and psychological health problems including breast pain, back pain, neck pain, shoulder pain and grooving, and intertriginous rashes. Respiratory restriction has also been suggested to be relieved after the bilateral breast reduction. A few previous studies on this topic were either a subjective analysis of patient comments or comparison of pulmonary function tests (PFTs) before and after reduction surgery.1-5 Besides the contradictory results of those reports, both “learning effect” of repeated PFTs and weight of removed specimen that diminishes the original body mass index (BMI) postoperatively might have also some effects on results. A few previous studies regarding the effect of reduction mammaplasty on pulmonary function tests reported improvements in PFTs after reduction mammaplasty, in the other hand some others reported contradictory results (1-5). Therefore, BMI may be the key linking whether a reduction mammmaplasty may affect PFTs, so it is worthwhile to investigate the relationship between bra cup size, BMI and PFTs in normal adult females. To contribute the solution of this conflict, we planned to evaluate the effects of breast size on pulmonary functions in a group of volunteer adult women. To the best of our knowledge, the effect of breast size on pulmonary function has not been shown in normal women population previously. MATERIALS AND METHODS Study design One hundred female volunteers without any known lung disease and recent or ongoing respiratory infection were enrolled into the study. Volunteers were all nonsmoker, older than 17 years old. None of them was pregnant, lactating, and had no breast or anterior chest wall operation. All the volunteers gave an informed consent, and ethical approval was obtained from the institutional board. Ages, weights, and underband and overbust measurements for breast sizes of subjects were recorded. Methods BMIs were calculated using the formula: weight/height2 (kg/m2). Obesity is defined as a BMI >30 kg/m2, and a BMI > 40 kg/m2 corresponds to morbid obesity.6,7 Cup sizes of breasts were calculated using a previously described method: differences between the overbust and underband measurements gave the cup sizes of participants.8 Four groups were formed according to the cup sizes as: <6.5 cm (cup size A), 6.5 to 13 cm (cup size B), 13 to 19.5 cm (cup size C), and >19.5 cm (cup size D). PFTs were conducted using spirometry instrument (Zan 200, PROV air II, Germany) in accordance with the criteria of American Thoracic Society.9 Firstly, the cases were told how the test was going to be carried out and the maneuver to be used was shown by conducting the test once more, when necessary. The cases put on nose clips in sitting position and were made to perform forced vital capacity maneuver. A maximum of five consecutive measurements were made and the results were recorded after choosing the best value. Tests carried out accordingly were assessed. The description and general interpretive significance of pulmonary function test parameters are as follows: forced vital capacity (FVC), the amount of air exhaled with as fast an expiration as possible after maximum inhalation. It is expressed in liters (l). FVC is related directly to changes in vital capacity. A reduction in FVC indicates primarily a restrictive type of pulmonary disorder. Forced expiratory volume in one second of FVC (FEV1) is the volume of air exhaled within one second from the start of a FVC maneuver. FEV1 is related to flow rates and disorders in the large airways. The ratio of FEV1 to FVC is FEV1/FVC. Forced expiratory flow rate over 25–75% of the forced vital capacity volume is FEF25–75(%) and peak expiratory flow rate is PEF. FEF25–75% is related to flow rates and disorders in smaller bronchi and larger bronchioles. Other parameters of forced expiratory flow (FEF25, FEF50, and FEF75) were recorded. A reduction in both FEV1 and FEV1/FVC parameters indicates an obstructive airway disease. Of the PFT parameters defined, measured liter (l) values and predicted percent (%) values were recorded for each case. Percent predicted values for each PFT parameter were calculated as follows:10 Percent predicted value = (actual value /predicted value) X 100. Statistical analysis Kolmogorov-Smirnov test confirmed a normal distribution pattern. To analyze the effect of breast size on lung function tests, Oneway ANOVA test was established and a p value < 0.05 was assumed as significant. Spearman correlation analysis was used to evaluate the relation between PFTs and BMI, and PFTs and breast size. RESULTS The mean age was 34.7±9.6 years (range, 18-53 years). The age distribution was homogenous between groups A, B, C, and D. The BMI ranged between 18.1 kg/m2 and 43.1 kg/m2 (mean, 28.3±6.2 kg/m2). There were 22 women in group A, 34 women in group B, 30 women in group C, and 14 women in group D. Forty-one volunteers had simple obesity (BMI > 30 kg/m2) and six volunteers had morbid obesity (BMI > 40 kg/m2) in our study. Distribution of age, BMI, and PFTs between groups is presented in table 1. No significant difference of PFTs was found between groups. Difference of BMI was significant between cup size groups (table 1). In the correlation analysis, no correlation was found between groups and lung function parameters. Age, BMI, and cup size were found in positive correlation with each other (p<0.05). BMI was negatively correlated with FEV1, FVC, FEV1/FVC, FEF50, and FEF25%. DISCUSSION Effect of reduction mammaplasty on pulmonary function has been questioned in a few previous studies. Conway and Smith performed a subjective observation and evaluated comments of patients for the improvement in breathing following bilateral breast reduction.1 They based their argument on increased chest compliance because of the reduction in breast size. Afterwards, lung function was assessed by PFTs before and after the bilateral reduction surgery and contradictory results were reported about the effects of reduction mammaplasty .2-5 Goldwyn2 studied PFTs before and after bilateral breast reduction surgery in 10 patients (mean specimen weight, 1980 g) and did not find any difference. Starley et al.,3 in their study with 19 women undergoing breast reduction, reported statistically significant postoperative improvement in pulmonary function, particularly parameters of peak expiratory flow rate, peak inspiratory flow rate, and forced vital capacity. The authors commented that there was an overall improvement in chest wall compliance and total compliance following breast reduction surgery. The mean weight of excised breast tissue in their study was 1546 g. Sood et al.4 demonstrated an improvement in inspiratory capacity, peak expiratory flow rate, and maximal voluntary ventilation. This also correlated positively with BMI; the more obese the patient was, the more the improvement there was in pulmonary function. According to those authors, the improvement in maximum voluntary ventilation implies that the reduction in breast mass improved overall chest wall compliance, thereby resulting in an improvement of dyspnea. The mean resection weight was 2220 g in that study. More recently, Iwuagwu et al.5 made a randomized comparative analysis and showed no significant difference in PFTs. However, they demonstrated a positive correlation between specimen weight resected (mean 1382 g) and FVC1/vital capacity (%); FEV/FVC; peak expiratory flow rate, and forced vital capacity. In contrary to previous reports, they found no correlation between BMI and PFTs possibly because that was not the main subject of their study. All of the patients in above mentioned studies (excluding the Conway and Smith who did not study PFTs) had PFTs within the normal limits before and after surgery, but the clinical significance of the improvements in test values beyond normal seems debatable. In addition, PFTs may be affected by patient weight and can be changed by learning (repeat tests). Both learning effect in repeated PFTs and weight of removed specimen that diminishes the original body mass index postoperatively have potential effects on the results of those studies. Perhaps the improvements in PFTs are related to BMI and if a female is morbidly obese and a reduction mammmaplasty leads to a decrease in bodyweight and BMI, than PFTs may improve also. In the present study, BMI was found in negative correlation with FEV1, FVC, FEV1/FVC, FEF50, and FEF25%. However, we found no correlation of these parameters with breast size. Women who have large breasts also have high body mass index as demonstrated in our study (table 1). In association with obesity, macromastia may lead to a relative restriction in chest wall compliance; therefore, reduction of breast size is expected to enhance chest wall compliance and lead to improved ventilation. Breast size contributes BMI, but it is not the only and most important constituent of it. Fat accumulation in other parts of the body including abdomen, chest wall, diaphragm, and extremities also increases the BMI.11 In the study of Sood et al.4 who showed improved PFTs after the surgery, mean BMI decreased to 30.8 kg/m2 from 31.4 kg/m2. We think that, this decrease might have an important role on the altered pulmonary function parameters. Starley et al.5 did not measured postoperative BMI and stated that their study sample was too small to relate these changes to mass of excised tissue or BMI. Reduction mammaplasty results a considerable weight loss that lowers the BMI. We think that a possible improvement in lung function after reduction mammaplasty may be secondary to decreasing BMI that is caused by resected specimen. Forty-one volunteers had simple obesity (BMI > 30 kg/m2) and six volunteers had morbid obesity (BMI > 40 kg/m2) in our study. It is previously demonstrated that chest wall compliance is relatively normal in simple obesity.12 In our study, low number of morbidly obese patients may be a limitation that caused insignificance of differences. A further study with a larger volunteer group including enough subjects from various body types will be beneficial. Breast size had no correlation with lung function in the present study that was performed with 100 healthy volunteer women aged between 18 and 53. Also, in previous studies about the effect of reduction mammaplasty, observed women had no respiratory illnesses.2-5 We think that our results may contribute to unravel the debate appeared by controversial results of previous reports. However, this may not the case for women with both respiratory disease and large breasts. Reduction mammaplasty may improve lung function associated with enhanced chest wall compliance in patients with respiratory disorders like asthmatics. This may be a subject of further studies. Main subject of our present study was the effect of breast size on lung function but not the effect of reduction mammaplasty. However, both methods focus on the same question: is lung function changed with large breasts? If so, an improvement of lung function would be expected with breast reduction. Regarding our findings and contradictory results in previous literature, as a matter of fact, breast reduction does not seem as a reliable way of improvement for pulmonary function in healthy women. Operative goals should be kept patient-centered and improvement of aesthetics and capacity of activity, pain relief, and ensuring self-confidence seem still the main objectives of reduction mammaplasty. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10031t1.jpg] |
| |||||||||

{kind=link}