 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
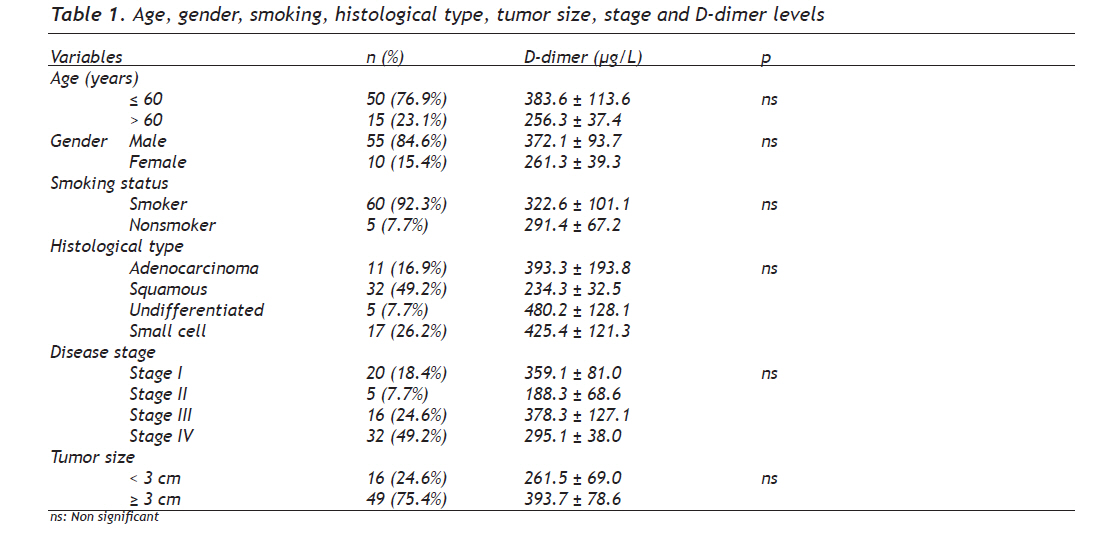
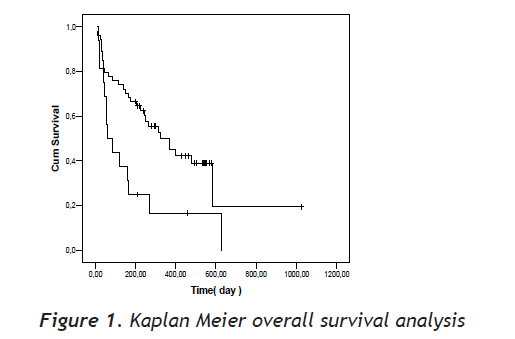
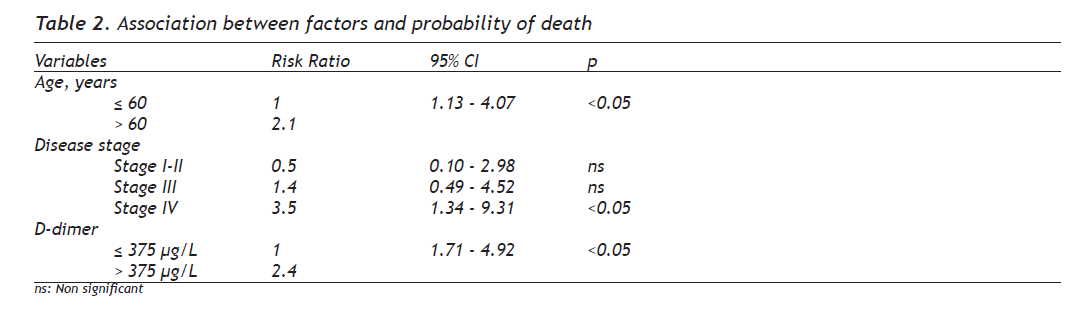
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 155-160 Original Article Prognostic Significance of Plasma D-Dimer Levels in Patients with Lung Cancer Akciğer Kanserli Hastalarda Plazma D-dimer Düzeylerinin Prognostik Değeri Ahmet Ursavaş, Mehmet Karadağ, Esra Uzaslan, Selma Yesilkaya, Funda Coşkun, Ercüment Eğe Uludag University, School of Medicine, Department of Pulmonary Medicine, Bursa, Turkey Received: 22.06.2009 Accepted: 14.11.2009 Correspondence: Ahmet Ursavaş, M.D, Uludağ Üniversitesi Tıp Fakültesi, Göğüs Hastalıkları Anabilim Dalı, 16059 Görükle/ Bursa/ Turkey, Phone: +902242950921, Fax: +902244428149 E-mail: ahmetursavas@gmail.com Code Number: gm10034 ABSTRACT Aim: Activation of coagulation and fibrinolysis pathways is frequently associated with malignancy. The objective of our study was to detect D-dimer levels in lung cancer patients and to determine whether there is any relationship between the stage of cancer and survival. Key words: Lung cancer, D-dimer Amaç: Malignitelerde koagülasyon ve fibrinolitik yolağın aktivasyonu sık görülür. Çalışmamızın amacı akciğer kanserli hastalarda D-dimer düzeylerini belirlemek ve kanser evresi, sürvi ve D-dimer düzeyleri arasındaki araştırmaktı. Anahtar kelimeler: Akciğer kanseri, D-dimer INTRODUCTION Haemostatic abnormalities can be present in more than 90% of cancer patients (1). The relationship between cancer and blood coagulation was first pointed out nearly one and a half centuries ago in the historical Trousseau publication (2). Activation of coagulation cascade frequently occurs in cancer via a number of mechanisms including the generation of tumor necrosis factor, tumor procoagulant and tissue factor (3). Patients with cancer may present with circulating markers of haemostatic activation such as shortened prothrombin time, partial thromboplastin time, increased levels of Factor II, V, VIII, IX, XI, XII, fibrinogen, Fibrinogen/fibrin degradation products, and the thrombin-antithorombin III complex. This hypercoagulable state may have an important role in the regulation of tumor growth and dissemination of cancer cells (4). In addition, the activation of coagulation pathway may contribute to cancer-induced angiogenesis (5). Fibrin turnover in the extracellular matrix of the tumor is essential for tumor angiogenesis and growth. Crosslinked fibrin in the extracellular matrix serves as a stable framework for endothelial cell migration during angiogenesis and tumor cell migration during invasion (6, 7). D-dimer is the degradation product of fibrin, resulting from the proteolytic action of plasmin. It is a sensitive marker of the fibrinolytic process. Elevated D-dimer levels have been detected in patients with thromboembolic events, disseminated intravascular coagulation, myocardial infarction, pneumonia and in vasoocclusive crisis in sickle cell disease (8-10). D-dimer levels also are elevated in patients with solid tumors including lung cancer. In addition, high plasma D-dimer levels is also associated with a large tumor burden, clinical progression, low rates of response to therapy, and poor prognosis in patients with lung cancer (11, 12). The objective of our study was to detect the D-dimer levels in lung cancer patients and to determine whether there is any relationship between the stage of cancer and survival. MATERIALS AND METHODS Patients Sixty-five patients with histologically or cytologically confirmed lung cancer treated at our institutions from January 2005 to April 2006 were enrolled in the study. Further eligibility criteria included having an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1 and a life expectancy of at least 3 months. Patients with active infection, another primary tumor, clinically significant cardiovascular, cerebrovascular or peripheral vascular disease, history of primary coagulation disease, recent or current use of anticoagulant drugs were excluded from the study. All subjects provided informed consent and the protocol was approved by the local Ethics Committee. Study Design The study was based on a prospective examination of blood coagulation tests in patients with lung cancer. All patients were classified according to the 1997 international system for staging of lung cancer (13). The instrumental evaluation included chest x-ray, fiberoptic bronchoscopy, computed tomography (of chest, adrenals, liver and brain). In potentially resectable tumors, mediastinal involvement was evaluated with mediastinoscopy. Patients with possible distant metastases were investigated with appropriate imaging studies or biopsies were obtained. Appropriate treatment modalities were recruited based on the clinical evaluation. Patients were followed up via phone calls to the patients themselves or their family members. Survival period was recorded as starting from the time of diagnosis to the date of death or termination of the study (April 2007). D-Dimer Assays Blood samples of lung cancer patients were drawn between 8:00 AM and 12:00 AM prior to the administration of any treatments. Plasma samples were stored at -20°C until the performance of assays. Commercially available reagents (Diagnostica Stago; Boehriger Mannheim, Mannheim, Germany) were used to measure D-dimer levels. The reference value for D-dimer was accepted as <375 μg/L. Statistical Analysis Statistical analysis was performed using the SPSS (Statistical Package for Social Sciences) for Windows, version 13.0. Concordance of normal distribution of all variables had been calculated with the Shapiro-Wilk test before comparison between OSAS and control groups. We used non parametric tests for dependent variables for the data that did not show normal distribution. Kaplan-Meier method was used for estimation of survival distribution. A P value less than 0.05 was considered as statistically significant. RESULTS Age, gender, smoking, histologic type, tumor size, stage and D-dimer Sixty-five patients with histologically or cytologically confirmed lung cancer were enrolled in the study. Mean age was 60.1 ± 10.5 years within the, range of 37-83 years, and there were 55 males (84.6%). There were no significant differences between males and females, young (<60 years) and old patients, smokers and nonsmokers when compared for D-dimer levels. There were 11 (16.9%) adenocarcinomas, 32 (49.2%) squamous cell carcinomas, 17 (26.2%) small cell carcinomas and 5 (7.7%) undifferentiated carcinomas. Twenty (18.4%) patients were classified as stage I, 5 (7.7%) patients as stage II, 16 (24.6%) patients as stage III, and 32 (49.2%) patients as stage IV. There was no significant difference between histological types and tumor stages in terms of D-dimer levels. Age, gender, smoking, histological type, tumor size, stage and D-dimer levels are shown Table 1. D-dimer mortality and survival analysis There were 23 (35.3%) dead and 42 (64.7%) alive patients at the termination of study. The plasma levels of D-dimer in the alive patients (216.3 ± 25.8 μg/L) were significantly lower than those of the dead group (406.5 ± 70.9 μg/L) (p <0.05). High plasma D-dimer concentrations were found to be a strong predictor of poor outcome (median survival period in patients with normal levels of D-dimer was 426 days [95% CI, 275-576 days] vs. 179 days [%95 CI, 68-289 days] in patients with increased levels; log rank statistics, 7.05; p <0.05, Fig 1). Results of cox regression analyses including age, stage and D-dimer levels are summarized in Table 2. Cox regression analyses showed that D-dimer (p < 0.05) was a prognostic factor independent of age and stage. DISCUSSION The results of the present study demonstrated that there were no significant relationships between plasma D-dimer levels and age, gender, smoking, tumor size histological type, and disease stage. However, high plasma D-dimer concentration was found to be a strong predictor of poor outcome, independent of age and tumor stage in patients with lung cancer. Interactions between the hemostatic system and cancer cells have been well established by several studies. Patients with cancer have a higher risk of developing venous thromboembolism. The mechanism of the hypercoagulation that occurs in cancer is complicated and a number of coagulation markers are disturbed (2-4). Furthermore, clinical and experimental studies support the notion that activation of coagulation / fibrinolysis may play an important role in the invasiveness of cancer (4, 14). D-dimer is a sensitive marker of the fibrinolytic process. Some data support the idea that tumors which activate the coagulation system to a higher degree behave biologically more aggressive and that the increased D-dimer levels may be associated with advanced tumor stage and poor prognosis (11, 12). The relationship between D-dimer levels and histological tumor types remains controversial. Seitz et al (12) reported that D-dimer was significantly increased in patients with metastatic disease; whereas Buccheri et al (15) demonstrated that there was no relationship between D-dimer levels and cell type, instead, D-dimer levels correlated with the stage of the disease. On the other hand, Unsal et al (16) reported that there were no significant differences among the histological types in terms of D-dimer levels. However they indicated that the group of patients with distant metastases (stage IV) had higher D-dimer levels compared to the other group without distant metastases (stage I-II-III). However, some other studies suggested that there is no relationship between tumor stage, histological type and D-dimer levels. A recent study also reported that there were no significant differences between D-dimer levels, tumor stage and histological type (17). In our study, we also found no significant differences between histological types and tumor stages when compared for D-dimer levels. Fibrin deposits may promote cell proliferation and neovascularisation of the growing tumor. Fibrin remodeling is involved in many steps of metastasis and has been proven have a critical role in the formation of new vessels. D-dimer is the smallest degradation product of fibrin, resulting from the proteolytic action of plasmin. Plasma levels of D-dimer may strongly predict survival and response to chemotherapy in lung cancer patients. Antoniou et al (18) measured plasma D-dimer levels in lung cancer patients before, during and after chemotherapy. They indicated that 73.7% of the patients with complete or partial response showed a reduction in plasma D-dimer levels and 68.8% of the patients with progressive disease showed increased D-dimer levels. Taguchi et al. (19) investigated plasma D-dimer levels in 70 lung carcinoma patients. They found that low levels of D-dimer were significantly predictive of both good prognosis and longer survival. Altiay et al (17) demonstrated that the median survival times were 207 to 405 days (p <0.001) for abnormally elevated and normal levels of plasma D-dimer respectively. Buccheri et al (15), reported the plasma levels of D-dimer in 826 lung carcinoma patients. The median survival time in the group with abnormally elevated D-dimer levels (154 days) was significantly lower than the group with normal D-dimer levels (308 days) (p <0.01). In the present study, we showed that the median survival period of patients with normal levels of D-dimer (426 days) was significantly higher than patients with increased values (179 days). The activation of coagulation in cancer patients has been implicated in both tumor progression and development of metastasis. The therapeutic use of anticoagulants might have a positive impact on the survival of cancer patients (20-24). Lee et al. (22) reported that low molecular weight heparin is superior to oral anticoagulation for the prevention of recurrence of venous thrombotic disease in cancer patients. Klerk et al (24) randomized 302 patients with advanced malignancy without venous thrombotic disease to low molecular weight heparin and placebo groups. They showed that mortality rate was significantly lower in the low molecular weight heparin group. Di Nisio et al (25) demonstrated that in patients treated with low molecular weight heparin, high initial D-dimer plasma levels were associated with a worse prognosis, and high D-dimer levels observed at the and of the 6 weeks of low molecular weight heparin treatment significantly correlated with reduced survival. In conclusion, we confirmed the prognostic value of D-dimer plasma levels in lung cancer patients, in accordance with the previous investigations. In addition, we demonstrated that D-dimer was a prognostic factor, independent of age and disease stages. We concluded that measuring plasma D-dimer may be helpful for predicting prognosis and risk of venous thrombotic disease in newly diagnosed lung cancer patients. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10034t1.jpg] [gm10034f1.jpg] [gm10034t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}