 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
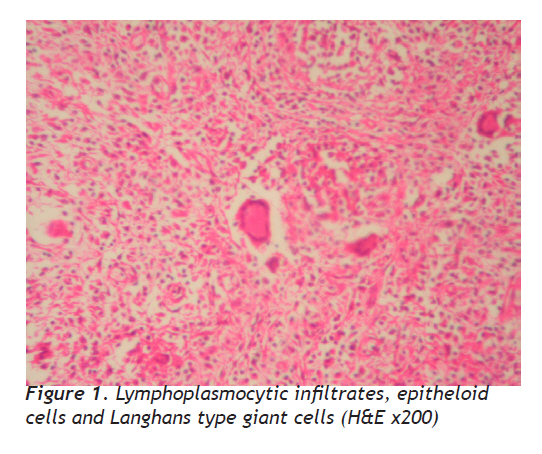
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 216-219 Case Report Tuberculosis of Breast Murat Kapan1, Mehmet Toksöz2, Şule Dönmez Bakır3, M. Erdal Sak4, Mehmet Sıddık Evsen5, Yaşar Bozkurt6, Akın Önder1 Dicle University Medical Faculty, Departments of General Surgery1, Gynecology5 and Urology6, 2Yeni Yaşam Hospital, Department of Radiology, Diyarbakır, 3Diyarbakır Training and Research Hospital, Department of Pathology, 4Ergani Public Hospital, Department of Gynecology, Diyarbakır, Turkey Received: 13.02.2009 Accepted: 09.05.2009 Correspondence: Dr. Murat Kapan, Dicle Üniversitesi Tıp Fakültesi, Genel Cerrahi Kliniği 21100-Diyarbakır, Tel: 0 412 2576410 E-mail: drmuratkapan@yahoo.com Code Number: gm10037 ABSTRACT Breast is one the least common location for tuberculosis (TB) infection and it may mimic breast cancer. Increasing prevalence of TB world¬wide may lead an increase in such uncommon manifestations of TB. In this report, we described two women with breast TB (34 and 28 years-old). Lumpectomy was performed to both patients due to suspicion of malignancy. Histological examination revealed characteristic tubercu-losis granulation tissue including epitheloid cells and Langhans type giant cells. Antituberculous therapy was given to both patients after surgical operation for 6 months and no complication was observed. In conclusion, TB should be kept in mind in the differential diagnosis of breast masses, especially in endemic tuberculous Key words: Tuberculosis, breast, extra pulmonary, surgical, treatment Meme Tüberkülozu Tüberküloz enfeksiyonun (TB) en az görüldüğü lokalizasyonlardan biri meme olup, meme kanserini taklit edebilir. Dünya çapında TB görülme sıklığında artış, TB’nin nadir klinik görünümlerinde artışa yol açabilir. Yazımızda meme TB’lu iki kadın hasta (34 ve 28 yaşında) sunulmuştur. Her iki hastaya malignite şüphesi nedeniyle lumpektomi uygulandı. Histopatolojik inceleme sonucunda Langhans tipi dev hücreler ve epiteloid hücreler içeren tüberküloza ait karakteristik granülasyon dokusu tespit edildi. Cerrahi sonrası her iki hastaya 6 ay boyunca antitüberküloz tedavi uygulandı ve herhangi bir komplikasyon görülmedi. Sonuç olarak; özellikle tüberkülozun endemik olduğu bölgelerde, meme kitlelerinin ayırıcı tanısında TB akılda tutulmalıdır. Anahtar kelimeler: Tüberküloz, meme, akciğer dışı, cerrahi, tedavi INTRODUCTION Although, tuberculosis (TB) is regarded as a pulmonary disorder; nearly 17.9% of TB cases have extrapulmonary manifestations (1). Breast is a rare site of extrapulmonary involvement. Breast TB, nearly 0.1% to 0.5% of all TB cases, is rare in Western Countries, incidence being 0.025% to 0.1% of breast lesions (2,3). However, the incidence of TB may be raising in developed countries, due to the increasing number of geriatric patients, especially those immunosupressed and due to the development of drug resistant strains of Mycobacterium tuberculosis (4). Breast TB usually affects young, multiparous, lactating women (4,5,6) and breast TB may represent the first manifestation of HIV infection (5). The most common clinical presentation of breast TB is a hard and irregular unilateral lump in the centrum or the upper outer quadrant of the breast, often associated with an inflammation of the overlying skin. Regional lymphadenopathy may be present in up to 15% of all cases (4,7). Breast TB is often difficult to differentiate from carcinoma or pyogenic abscess (3,7). Other granulomatous lesions such as sarcoidosis, various fungal infections, and granulomatous reactions to altered fatty material should also be excluded (3). Herein we reported two cases of breast TB, to attract attention to breast TB which is an uncommon disease mimicking carcinoma of breast. Case 1 A 34 year-old woman presented with a four months history of right breast mass. There was no history of oral contraceptive use and family history of breast cancer. The patient had five children. The smallest one is 2 years old and still not breast-fed. On physical examination, an irregular, hard, painful and mobile mass, 6 cm in diameter, coexisting with edema and erythema of breast skin was found in the lower inner quadrant of her right breast. There was skin retraction, but neither nipple discharge nor palpable axillar lymph nodes was found. All vital signs, as well as results of blood and urine analysis and chest X-ray were normal. CA-125, CA 15-3, AFP and CEA levels were within normal limits. Her total leukocyte count was 9.900/mm3 with 72.5% neutrophils. Erythrocyte sedimentation rate was 52 mm/hour (N, 0-20 mm/hour). Ultrasound (USG) showed 6 x 6 cm diameter, hypoecogenous, heterogenic mass in the lower inner quadrant of the breast. Mammography was performed and showed 6 cm diameter irregular mass without regional lymph nodes involvement. No abnormality was found in thoracic CT examination. Based on the physical examination and results of USG and mammography, the patient underwent lumpectomy with suspicion of malignancy. Intraoperatively, we noticed that the lesion was purulent and thought that it might be an abscess. The culture of purulent discharge remained sterile. Histopathological examination of the tissue revealed tuberculosis granulamatous lesions which consisted of fibrous and lymphoid tissue infiltrated by large epitheloid granulomas with central acellular necrosis and many giant cells, indicating the diagnosis of TB infection. After diagnosis of TB, the patient received anti-tuberculosis therapy with daily doses of 1200 mg Ethambutol (E), 600 mg isoniazid (H), 450 mg Rifampicin (R) and 1500 mg Pyrazinamide (Z) for 2-months and followed four months with 600 mg isoniazid (H), 450 mg Rifampicin (R) (2EHRZ\4HR). No side effect or complication recorded. The patient had an uncomplicated postoperative period. Case 2 A 28 year-old woman presented with a 3-month history of left breast mass. No history of oral contraceptive use, and family history of breast cancer were detected. She had three children and the last delivery was 6-months ago. On physical examination, an irregular, hard, painful and mobile mass, 5 cm in diameter, in the upper outer quadrant of her left breast with coexisting edema, erythema and retraction of the skin was detected. Areola and nipple were found to be normal. Enlarged lymph nodes in the left axilla, the biggest one being 1.5 cm diameter, was detected with manual examination. All vital signs, as well as results of blood and urine analysis and chest X-ray were normal. CA-125, CA 15-3, AFP and CEA levels were normal. Her total leucocyte count was 12.900/mm3 with 69.9% neutrophils. Erythrocyte sedimentation rate was 43 mm\hour ( 0 – 20 mm/hour). Ultrasonography showed a 3x2 cm diameter of hypoechoic, heterogeneous mass in the outer upper quadrant of the breast. Breast skin was edematous and thickened at this segment. There were 3-4 lymph nodes in the left axilla and the largest one was 13 mm in diameter. Our first diagnosis was a breast abscess. Mammography showed a 4 cm diameter irregular mass (BI-RADS 5). There were 3-4 regional lymph nodes. No abnormal imaging finding was seen in Thoracic CT examination. Fine-needle aspiration cytology (FNAC) was performed from the breast lesion and the axillary lymph nodes. Acute inflammatory exudates dominated in the FNAC cytology and the examination of lymph node revealed a reactional inflammation. For preoperative inhibition of lactation, the patient had taken Kabergolin treatment with 0,5 mg daily dose for two days (1 mg totally) one week prior to the surgery. Because of suspicion for malignancy, the patient underwent lumpectomy. The culture of purulent discharge remained sterile. Histopathological examination of the tissue, which measured 10x7x4 cm in diameter, revealed tuberculosis granulation tissue. The patient was subjected to a six month course of anti-tuberculosis treatment with daily doses of 1200 mg Ethambutol (E), 600 mg isoniazid (H), 450 mg Rifampicin (R) and 1500 mg Pyrazinamide (Z) for two months , followed by four months with 600 mg isoniazid (H), 450 mg Rifampicin (R) (2EHRZ/4HR). No side effect or complication was seen. DISCUSSION Tuberculosis of the breast is a rare disease with incidence ranging from 0.1% in developed countries and up to 0.3-5% in endemic regions (2). Turkey is one of the endemic regions for tuberculosis, with a reported incidence in the general population as 43-46/100.000, especially in the east and southeast of Turkey (8). Tuberculosis of breast is rare because breast is not a suitable site for multiplication and survival of tubercle bacilli (9). Women in the younger age group are more often affected. Most cases are 20 to 40 years old women in active sexual life, since at this period of life breast experience more physiological changes and is more susceptible to trauma and infection. In pregnant and lactating women, the breast is vascular with dilated ducts predisposed to trauma making it more susceptible to tuberculosis. Also tuberculosis of male breast has been reported very rarely (2-5,10-12), both of our patients were female, 34 and 28 years old, and one of them lactating. Breast tuberculosis may be primary or secondary. Secondary infection may occur as a result of hematogenous spread, retrograde spread from axillary lymph nodes or direct extension from the lung, pleura, mediastinum and articular lesions (4,13). But the most accepted view for spread of infection is centripedal lymphatic spread (3,5,10). The ipsilateral axillary and cervical lymph nodes are affected in the majority (50—70%) of cases, suggesting breast involvement following retrograde lymphatic extension (5). In one of our patient, we did not find any focus except breast. In the other one, ipsilateral axillary lymph node was positive for TB. Most common clinical presentation of breast tuberculosis is a lump, an abscess, a single or multiple discharging sinuses (4,10,14). The commonest location of the lumps is the centrum or upper outer quadrant of the breast (4,10,14,15). The mass may be fluctuated and is usually covered with indurated tissue and fixed to the skin. Nipple and skin retraction can also occur. But fistulization and pain is not uncommon (4,10,14). One of our patient’s lump was in the upper outer quadrant of her left breast, the other’s was in the lower inner quadrant of her right breast. Both of them had coexisting edema, erythema of the skin and skin retraction, but neither nipple discharge nor fistulization were observed. One of them had an enlarged lymph node in axilla. Based on radiological and clinical characteristics, breast TB is newly classified as nodular, disseminated, and abscess varieties. Most common form is the nodular form (3-5,14,15). Our two cases had also nodular form. Imaging modalities, like mammography or USG are of limited value in the differential diagnosis. With these imaging methods, it is difficult to distinguish the lesion from breast carcinoma (3,14,15). Computed tomography and magnetic resonance imaging are not diagnostic, but may reveal the extent of involvement for surgery (3,14). In our patients, the imaging methods could not differentiate breast tuberculosis from breast cancer. The gold standard fort the diagnosis breast TB is definition of M.tuberculosis by Ziehl-Neelsen staining or by culture. But histochemistry is not practical and culture of TB has some limitations. So FNAC may be the other important practical method for diagnosis (5). However, FNAC from the breast lesions can not determine the etiologic agent, but definition of both epitheloid cell granulomas and necrosis is enough for the diagnosis of breast TB, leading to definitive diagnosis in up to 73% of cases (5,6,15). However failure to demonstrate necrosis on FNAC does not exclude breast tuberculosis Nucleic acid amplification tests (NAAT) such as polymerase chain reaction (PCR) are rapid and specific, but its sensitivity is low especially in AFB smear negative cases (15). PCR is recommended in cases in which culture is negative or for differential diagnosis between other forms of granulomatous mastitis (6). The Tuberculin skin test, interferon gamma release assays and serology are of limited diagnostic values (15). In our patients, the last one underwent FNAC. FNAC revealed predominately acute inflammatory exudates and the reactional lymph node. We did not perform the other tests, because of limited technical facilities of our laboratory. There are various modes of therapies including anti-tuberculosis chemotherapy and mastectomy for breast tuberculosis. Nowadays suggested therapy is incisional or excisional biopsy combined with anti-tuberculosis drugs (1,3,12). Anti-tuberculosis treatment includes; 6 months therapy impending 2 months’ intensive phase and followed by 4 months continuation phase. Anti-tuberculosis drugs are 1200 mg ethambutol (E), 750 mg streptomycin (S), 450 mg rifampicin (R), 600 mg isoniazid (H) and 1500 mg pyrazinamide. (3,15). Our patients underwent lumpectomy. Histopathological evaluation revealed breast tuberculosis. Afterwards 2 months EHRZ\4 months HR protocol had given to the patients. In our patients no side effect or complication were observed In conclusion, breast tuberculosis is a rare disease, which is difficult to differentiate clinically and radiologically from breast cancer and abscess. Breast tuberculosis can be treated with anti-tuberculosis chemotherapy in early stages, but in late stages the most successful therapy is incisional or excisional biopsy together with anti-tuberculosis chemotherapy. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10037f1.jpg] |
| |||||||||

{kind=link}