 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
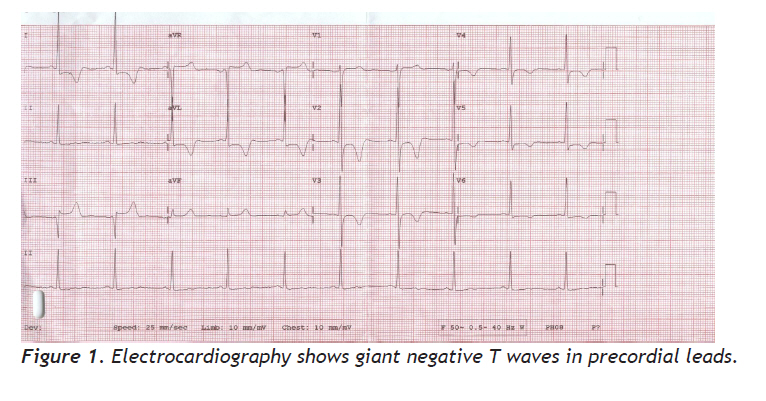
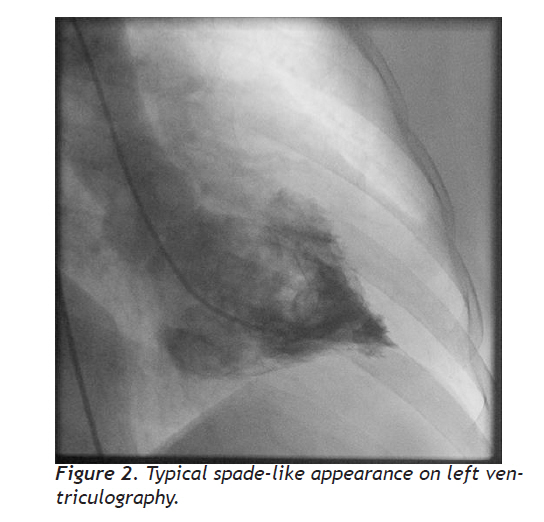
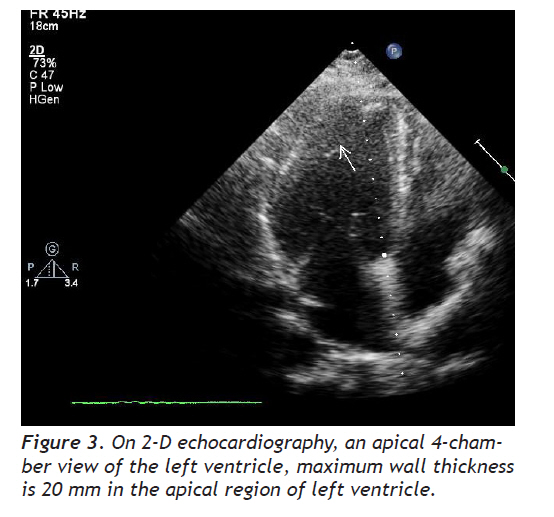
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 206-209 Case Report Apical Hypertrophic Cardiomyopathy Apikal hipertrofik kardiyomyopati Makbule Nur Yıldırım,Yusuf Selçoki, Beyhan Eryonucu Fatih University, Faculty of Medicine, Department of Cardiology, Ankara, Turkey Correspondence: Makbule Nur Kankilic, Department of Cardiology Medical Faculty of Fatih University Alparslan Turkes Caddesi, No: 57, 06510, Emek, Ankara, Turkey Phone: +90 505 4505951, +90 312 2035083 Fax: +90 312 2213670 E-mail: mnkankilic@gmail.com Received: 18.02.2009 Accepted: 07.08.2009 Code Number: gm10038 ABSTRACT Apical hypertrophic cardiomyopathy (AHCM) is one form of hypertrophic cardiomy¬opathy that is the most common hereditary cardiac disease and the most frequently found cardiomyopathy. AHCM has typical findings on electrocardiography, echocardiography and ventricu¬lography. The electrocardiographic changes and symptoms associated with AHCM often mimic acute coronary syndromes and coronary angiogram can be performed with pre-diagnosis of coronary artery disease several times. Physicians should consider AHCM in case of patients who have similar electrocardiographic changes and symptoms with coronary artery disease. Key words: Apical, hypertrophic, cardiomyopathy Apikal hipertrofik kardiyomyopati (AHCM), en sık gözlenen kalıtsal kalp hastalığı ve kardiyomyopati olan hipertrofik kardiyomyopatinin bir formudur. AHCM elektrokardiyografi, ekokardiyografi ve ventrikülografide tipik bulgulara sahiptir. Elektrokardiyografik bulgular ve semptomlar akut koroner sendromları taklit edebilir ve koroner arter hastalığı ön tanısı ile koroner anjiyografi birkaç kez yapılabilir. Koroner arter hastalığı semptom ve elektrografik değişiklikle başvuran hastalarda AHCM tanısı akla gelmelidir. Anahtar kelimeler: Apikal, hipertrofik, kardiomiyopati INTRODUCTION Hypertrophic cardiomyopathy is the most common hereditary cardiac disease and the most frequently found cardiomyopathy (1). Apical hypertrophic cardiomyopathy that is one form of hypertrophic cardiomyopathy is characterized by primary hypertrophy localized in the apex of the left ventricle (2). The apical form of hypertrophic cardiomyopathy was first reported in Japan by Sakamoto et al.(3) and subsequently by Yamaguchi et al. (4) This condition is common in Japan and estimated to represent 25% of Japanese patients with hypertrophic cardiomyopathy, whereas, in non-Asian patients, the insidence of apical hypertrophic cardiomyopathy does not exceed 1-2 % (5). Apical hypertrophic cardiomyopathy has typical findings on electrocardiography, echocardiography and ventriculography. The electrocardiography in apical hypertrophic cardiomyopathy shows giant T wave negativity which is defined as a voltage of negative T wave ≥1 mV (≥10 mm) in any of the leads and high R wave voltage. Angiographic feature of apical hypertrophic cardiomyopathy is end-diastolic LV cavity configuration resembling an ‘ace of spades’. The mid-ventricular obstruction was also demonstrated by transtorasic Doppler echocardiography (6). Although apical hypertrophic cardiomyopathy has been reported to have a benign prognosis, one-third of apical hypertrophic cardiomyopathy patients may have severe complications such as myocardial infarction, atrial fibrillation and stroke (6). The electrocardiographic changes and symptoms associated with apical hypertrophic cardiomyopathy often mimic acute coronary syndromes (7). Here we report a case of apical hypertropic cardiomyopathy with symptoms and electrocardiographic findings mimicking ischemic heart disease. CASE A 46-year-old woman suffering from chest pain and progressive dyspnea on exertion was admitted to our hospital. She had the symptoms for 2 months. She undergone coronary angiogram with these symptoms and electrocardiography changes three years ago. Her coronary risk factors included a history of hyperlipidemia and premature atherosclerosis in her mother. Physical examination was normal. Her electrocardiography showed giant negative T waves in precordial leads (8) (Figure 1). Because of the symptoms, electrocardiography findings and risk factors of coronary artery disease, we performed a coronary angiography. It was determined that the patient had normal coronary arteries and typical spade-like appearance on left ventriculography (Figure 2). On 2-D echocardiography, an apical 4-chamber view of the left ventricle revealed hypertrophy of apex and maximum wall thickness was measured as 20 mm in the apical region of left ventricle (Figure 3). The patient was diagnosed of apical hypertrophic cardiomyopathy and treated with beta blocker. DISCUSSION Apical hypertrophic cardiomyopathy has a significant proportion of the overall hypertrophic cardiomyopathy. In general, apical hypertrophic cardiomyopathy has a benign prognosis. Patients present with typical findings on electrocardiography, echocardiography and ventriculography. Cardiac catheterization is frequently performed in these patients. Because of electrocardiography findings, coronary angiogram can be performed with pre-diagnosis of coronary artery disease several times. In our case, coronary angiography was performed for the suspicion of coronary artery disease for the second time. We diagnosed apical hypertrophic cardiomyopathy after cardiac catheterization, an invasive procedure. The electrocardiographic changes in our case were related with apical hypertrophic cardiomyopathy. On 2-D echocardiography, an apical 4-chamber view of the left ventricle revealed hypertrophy of apex, the maximum apical wall thickness was 20 mm. Duygu et al. have shown that mean maximum apical wall thichness was 18 mm in seventeen patients (6). The study of Kitaoka et al. demonstrated that wall thickness at the apex was greater in American patients than in the Japanese patients (23±4 vs. 18±2 mm, respectively) (9). In patients with apical hypertrophic cardiomyopathy, a transtorasic echocardiogram may not show the hypertrophy localized to the apex. In adition the apex can be demonstrated by transesophageal echocardiography. If echocardiographic images are inadequate, magnetic resonance imaging may be used to diagnose apical hypertrophic cardiomyopathy. In some cases apical hypertrophy may be confused with apical trombus. Differentiation of these conditions can be done by myocardial contrast echocardiography. In this technique, a contrast agent is injected intravenously to highlight hypertrophied myocardium by echocardiography. In conclusion, physicians should consider apical hypertrophic cardiomyopathy in case of patients who have similar electrocardiographic changes and symptoms with coronary artery disease. Adequate diagnostic methods are needed to distinguish between apical hypertrophic cardiomyopathy and coronary artery disease. Although echocardiography remains the first choice for investigation, cardiac magnetic resonance imaging can be performed (10). Differentiation of apical hypertrophy from unstable angina and apical thrombus/other masses can be done by use of further imaging modalites. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10038f2.jpg] [gm10038f3.jpg] [gm10038f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}