 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
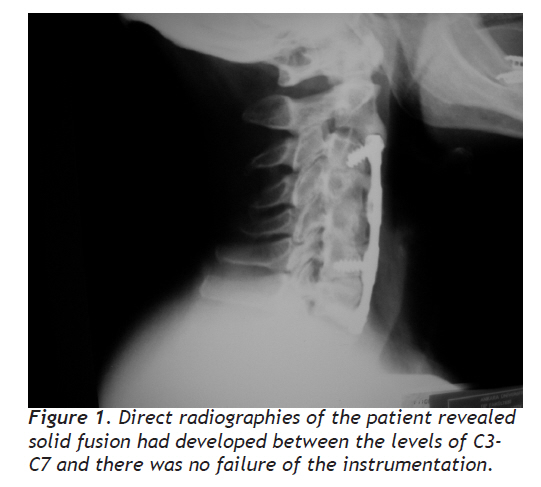
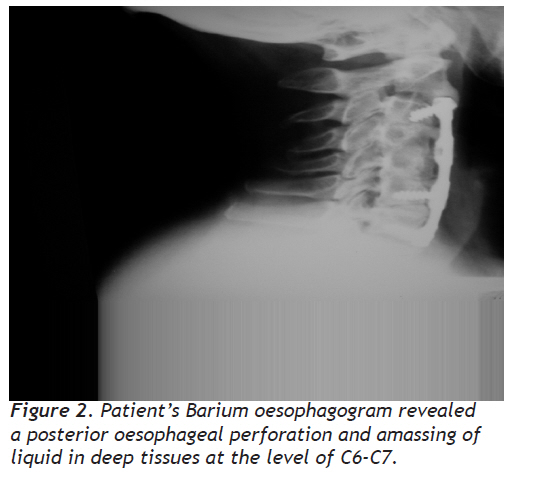
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 210-212 Case Report Esophageal Perforation Due to Revision of Anterior Cervical Spine Surgery Anterior Servikal Omurga Cerrahisi Revizyonuna bağlı Özafagus Perforasyonu Cem Yılmaz, Serdar Kabataş, Salih Gülsen, İlker Coven, Hakan Caner Baskent University School of Medicine, Department of Neurosurgery, Ankara, Turkey Correspondence: Serdar Kabatas, MD, Baskent University School of Medicine Istanbul Hospital, Department of Neurosurgery. Oymaci Sokak No:7 34662 Altunizade/ Istanbul/ Turkey, Tel: +902165541500 ; Fax: +902166519746 E-mail: kabatasserdar@hotmail.com; serdark@baskent-ist.edu.tr Received: 15.01.2009 Accepted: 07.08.2009 Code Number: gm10040 ABSTRACT Oesophageal perforation is a rare but potentially life threatening complication due to anterior cervical spine surgery (ACSS). In this report, we present a 55-year-old woman with a complication of oesophageal injury following an ACSS with a successful outcome. Key words: Anterior cervical spine surgery, complication, oesophageal perforation Abbreviations: Anterior cervical spine surgery (ACSS), Cerebrospinal fluid (CSF), Magnetic resonance imaging (MRI), Ossification of posterior longitudinal ligament (OPLL), Percutaneous endoscopic gastrostomy (PEG), Ultrasonography (USG) Özafagus perforasyonu nadir fakat anterior servikal omurga cerrahisine (ASOC) bağlı potansiyel olarak yaşamı tehdit eden bir komplikasyondur. Bu yazıda, ASOC sonrasında özafagus yaralanması komplikasyonu gelişen ve başarıyla tedavi edilen 55 yaşındaki bir kadın hastayı sunduk. Anahtar kelimeler: Anterior servikal omurga cerrahisi, komplikasyon, özafagus perforasyonu INTRODUCTION Anterior approach to the cervical spine has gained wide acceptance among both neurosurgeons and orthopaedic surgeons for the treatment of cervical degenerative spondylosis, disc herniation, ossification of posterior longitudinal ligament (OPLL), tumours and trauma. Plates and screws are usually used to achieve further stabilization of the cervical spine; however, they can also increase the complication rates (1). Complications seen in anterior cervical spine surgery (ACSS) include recurrent nerve damage, Horner syndrome, spinal cord contusion, nerve root lesions, haematoma, superficial/ deep wound infection, cerebrospinal fluid (CSF) fistula, meningitis, and oesophageal and hypopharingeal perforation (1,2). Iatrogenic perforation of cervical oesophagus or hyphopharinx is a rare and life threatening complication since it may result in descending mediastinitis. Here, a case of an iatrogenic perforation of cervical oesophagus due to ACSS is presented. CASE A 55–year-old patient was admitted with dysphagia and neck pain. The patient recounted a history of an anterior cervical discectomy and fusion between the level of C3-C7 with an anterior cervical plate and screws for five years ago. Cervical magnetic resonance imaging (MRI) and direct radiographies of the patient revealed solid fusion between C3 and C7 vertebra levels and there was no failure of the instrumentation (Figure 1). Although there was no objective criteria, the patient requested her screws and plate to be removed. The patient was operated on, and the cervical plate and screws were removed. She was discharged at the second postoperative day with no complaints. One week after the operation, the patient was readmitted with complaints of dysphagia and fever. She reported that her neck was swelling after drinking water. On examination, she had erythema and oedema formation on the wound. Superficial ultrasonography (USG) revealed subcutaneous emphysema. Barium oesophagogram revealed a posterior oesophageal perforation at the level of C6-C7 (Figure 2). Conservative treatment with broad spectrum intravenous antibiotics and feeding through a percutaneous endoscopic gastrostomy (PEG) was instituted. The patient was not given oral diet for one week and the oesophageal perforation was left to heal spontaneously. The control barium oesophagogram taken after 10 days revealed that the perforation was healed and she was started oral feeding. The patient was well without any complaints on the follow-up examination after six months. DISCUSSION Complications associated with ACSS are rare and mostly related to the complex anatomy of the cervical region. Due to the close anatomical relationship, the oesophagus and pharynx are at occasional risk for perforation. The reported incidence of oesophageal injuries ranges between 0 and 3.4% and they are either recognized intraoperatively and called early injuries, or recognized some time after the operation and called delayed injuries (3, 4). In the early cases, the mechanism of the injury is usually related to sharp dissection, retractor blades, direct surgical injury or traumatic endotracheal intubation. On the other hand, delayed cases can manifest themselves many years after surgery and are usually related to chronic compression, dislocation or migration of the bone graft or internal fixation materials (5). In our case, the oesophagus was injured intraoperatively, but it could not be recognized until the postoperative first week. At that time, the patient was readmitted with dyphagia, fever and neck swelling after drinking water. On examination, she had erythema and oedema formation on the wound. Although dysphagia is a common symptom following ACSS, wound infection and neck swelling after drinking water are pathognomonic symptoms of oesophageal injury. Other symptoms that should raise suspicion would be neck and throat pain, aspiration, unexplained tachycardia and blood in the nasogastric tube (3). To confirm this diagnosis, superficial USG was performed and subcutaneous emphysema was determined. Subcutaneous emphysema detection on either USG or plain X-ray is also reported to be pathognomonic. Eventually barium oesophagography was obtained to ensure the exact location of perforation. It revealed that the perforation was at the C6-C7 level which is one of the most common levels of occurrence of oesophageal perforation together with C5-C6 level. It is reported that the cricopharyngeal region at the level of C5-C6 where the oesophagus lies directly on the spine and only covered by fascia posteriorly is crucially at risk. Revision surgery is also reported to be a risk factor for this type of oesophageal injury because of paravertebral soft tissue fibrosis, which we thought may be the cause in our case (3). The treatment of oesophageal perforation depends on the timing of the recognition of injury. If the perforation is detected at the time of the surgery, simple suturing would solve the problem. If recognised in the first hours or days following surgery, simple suturing with irrigation and drainage of the operative field to avoid infection is necessary. Furthermore, if the perforation size is large, sternocleidomastoid or omohyoid muscle flaps can be used. Any abscess or wound infection must be treated with antibiotics. Neverthless, there has been much debate over the treatment of late diagnosis. While some surgeons believe that simple drainage and conservative treatment is enough, others believe that up to 25% of patients treated consevatively develop a cervical abscess and surgery must be performed whenever possible to avoid this (5). They recommend that conservative treatment must be restricted to small and undetectable perforations. In our case, the perforation was small, however detectable, therefore, conservative treatment along with feeding through PEG for one week was enough to allow spontaneous healing of the perforation. Oesophageal perforations should be followed up for late sequelae, like strictures and diverticula. Our patient had no problems six months after the treatment. In conclusion, although oesophageal perforation is a rare complication seen after ACSS, it is a potentially life threatening problem because of the risk of descending mediastinitis. The most important diagnostic tool is a high level of suspicion in such cases presenting with acute dysphagia after cervical surgery. Treatment can be either by primary suturing or simple drainage with or without stopping feeding through the orogastric route, and allowing spontaneous healing depending on the size of perforation and time of presentation and/or detection of the problem. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10040f2.jpg] [gm10040f1.jpg] |
| |||||||||

{kind=link}
{kind=link}