 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
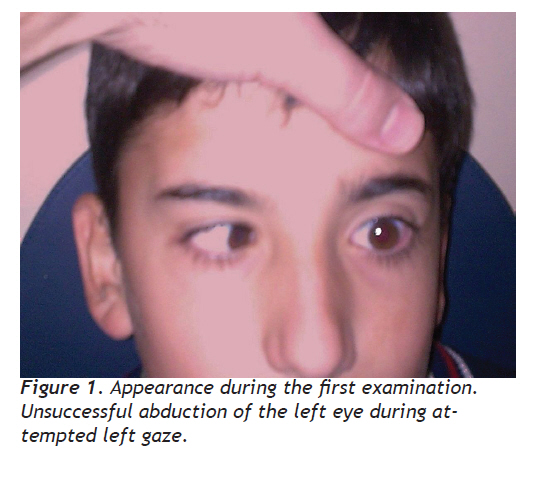
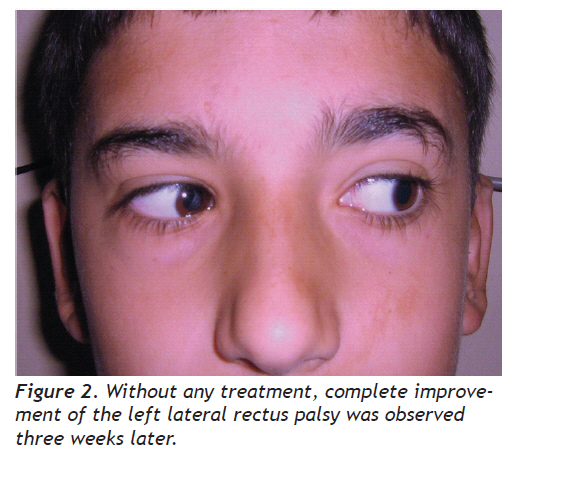
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 220-222 Case Report Benign Isolated Abducens Nerve Palsy Benign İzole Abdusens Siniri Felci Murat Özdemir, Mesut Garipardiç Kahramanmaraş Sütçü İmam University, Faculty of Medicine, Departments of Ophthalmology and Pediatrics, Received: 02.04.2009 Accepted: 21.05.2009 Correspondence: Dr. Murat Ozdemir Kahramanmaras Sütçü İmam University, Faculty of Medicine, Department of Ophthalmology 46100, Kahramanmaraş, Turkey Phone: +903442212337 Fax: +903442212371 E-mail: drmozdemir@hotmail.com Code Number: gm10041 ABSTRACTCranial nerve VI (abducens nerve) innervates the lateral rectus muscle. Acquired isolated abducens nerve palsy in infants and children is a rare condition. A lesion of abducens nerve will result in esotropia greater at distance, an ipsilateral abduction deficiency, and a double vision. The abducens nerve palsy in a child may be caused by serious neurological diseases such as raised intracranial pressure, tumors, or tuberculous meningitis. However, the abducens nerve palsy can rarely occur in children after minor febrile episodes or upper respiratory infections, and that is named as benign sixth nerve palsy which is generally reversible. In this report, we discussed the diagnostic and therapeutic approach in a pediatric case had a benign isolated abducens nerve palsy. Key words: Abducens nerve palsy; Diplopia; Paralytic strabismus Altıncı kafa siniri (abdusens siniri) dış rektus kasını innerve eder. Bebeklerde ve çocuklarda, sonradan oluşan izole abdusens siniri felci çok nadir bir durumdur. Abdusens felci özellikle uzağa bakışta ortaya çıkan içe kayma, o tarafta dışa bakış kısıtlılığı ve çift görmeye neden olur. Çocuklarda abdusens siniri felci kafa içi basınç artışı, tümörler veya tüberküloz menenjiti gibi çok ciddi durumlarla birlikte olabilir. Bununla birlikte, abdusens siniri felci çocuklarda çok nadiren hafif ateşli bir hastalık veya üst solunum yolu enfeksiyonundan sonra da ortaya çıkabilir. Bu durum genellikle geri dönüşümlü olup benign altıncı sinir felci olarak adlandırılır. Bu sunumda, benign izole abdusens siniri felci olan bir olguda tanı ve tedavi yaklaşımını tartıştık. Anahtar kelimeler: Abdusens siniri felci, çift görme, paralitik şaşılık INTRODUCTION The abducens nerve, the sixth cranial nerve, innervates the lateral rectus muscle of the eye and is responsible for lateral horizontal ocular movement. An abduction deficit, which may be complete (palsy) or incomplete (paresis), results in esotropia, ipsilateral abduction deficiency, and double vision. Patients will report diplopia that is worse at distance and when looking toward the affected muscle. A lesion anywhere along the abducens nerve course, from the pons to the orbit, can cause a paresis or palsy. Abducens nerve palsy can be associated in children with different clinical pictures underlying significant pathology. Prompt and correct diagnosis by an eye care practitioner is critical in determining the cause and, therefore, the proper evaluation, follow-up, and treatment. The abducens nerve palsy in a child raises the suspicion of serious neurological disease-raised intracranial pressure, an infiltrating glioma of the pons, and tuberculous meningitis being possibilities (1,2). However, “the benign six-nerve palsy” described firstly by Knox et al (3) can rarely occur in children after minor febrile episodes or upper respiratory infections. In this report, we discussed the diagnostic and therapeutic approach a pediatric case had a transient abducens nerve palsy occurred after an upper respiratory infection. CASEA 12-year-old boy presented with a sudden onset of double vision. He denied any recent head or neck trauma, headaches, fevers, or nausea. A review of systems was also negative for any weakness, aphasia, confusion, ataxia, vertigo, or dysphagia. The patient’s past medical history was significant only for upper respiratory infection two weeks ego (probably viral), but he was not taking any medications. He denied tobacco or illicit drug use. There was no family history of any neurological disorders. On examination, he had obvious left-sided head position. Left lateral gaze palsy was evident (Figure 1) while the rest of the central nervous system examinations were within normal limits. A non-contrast and contrast magnetic resonance imaging (MRI) scan of the head and neck confirmed normal brain and orbital structures. We thought benign isolated sixth-nerve palsy in left eye. We suggested the patching for left eye to prevent a double vision, and followed the patient by one-week interval. At two weeks after the diagnosis, the double vision disappeared and lateral gaze palsy resolved partly. The condition was improved completely at three weeks (Figure 2). DISCUSSIONIn its long and tortuous course from pontine somatic motor nucleus, the abducens nerve runs through different anatomic structures including subarachnoid space, temporal bone, cavernous sinus, and orbit and thus is susceptible to a variety of insults. Lateral rectus palsy is usually caused by tumors, hemorrhages, head trauma, and inflammations such as meningitis, Miller Fisher syndrome, and Gradenigo’s syndrome and may rarely occur as a complication of ophthalmoplegic migraine (1,2,4) Benign isolated abducens nerve palsy is a rare clinical entity characterized by spontaneous resolution within 6 months. Diagnosis is determined retrospectively after exclusion of the main conditions of sixth nerve palsy in childhood, and is different from benign recurrent forms. The first description dates back to Knox et al. who in 1967 reported 12 children who presented with a sixth nerve palsy as their main symptom; three of them had a prior history of otitis media and then were affected with Gradenigo syndrome, whereas for the other nine patients the investigators assumed that the benign palsy was due to antecedent viral febrile or upper respiratory illness (3). The etiology of benign isolated six-nerve palsy remains uncertain. The authors suggest that it may be comparable to Gradenigo’s syndrome, in which otitis media is complicated by an ipsilateral sixth-nerve lesion. Any finding of otitis media did not detected in our case. The alternative explanation for the benign palsies is that the nerve lesion is due to a viral neuritis (3). This theory may be explain in our case. Several viral or bacterial agents reported in the literature were correlated to isolated abducens palsy. Particularly some reports were described secondary to immunizations (measles, measles-mumps-rubella, diphtheria-tetanus-pertussis vaccines), others to Epstein-Barr, varicella, herpes zoster ophthalmicus, Mycoplasma pneumoniae, Chlamydia pneumoniae, and cytomegalovirus infections (5). Knox et al (3) suggested that if there is a history of a preceding febrile illness and if there are no other abnormal neurological signs, normal x-rays of the skull and sinuses, no abnormality in the cerebrospinal fluid, and no response to pharmacological tests for myasthenia gravis, it is reasonable to delay other investigations and keep the child under observation for three to six weeks, when improvement should be starting if he is suffering from this type of benign sixth-nerve palsy. Currently, computerized tomography (CT) and MRI investigations can be easily performed almost anywhere. In this cases, we suggest that CT and/or MRI investigations should be performed in addition to Knox et al’s suggestions and if it can nor be found an underlying etiology, benign six nerve palsy should be thought and the patient should be followed for three to six weeks without any treatment. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10041f1.jpg] [gm10041f2.jpg] |
| |||||||||

{kind=link}
{kind=link}