 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
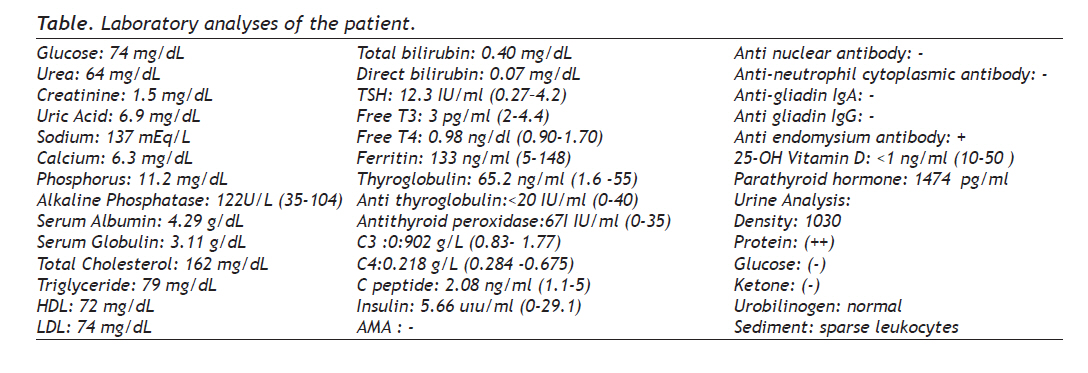
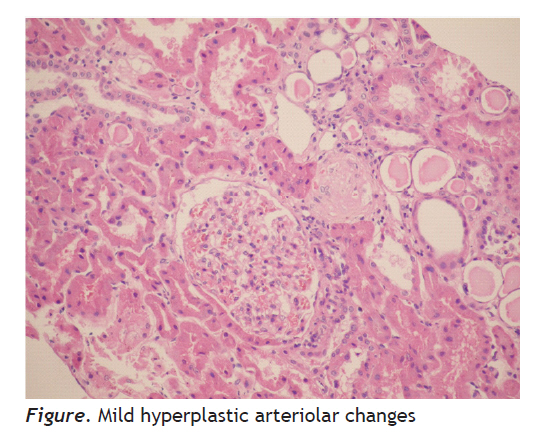
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 226-229 Case Report Celiac Disease Complicated with Renal Insufficiency and Autoimmune Thyroid Disease Otoimmün Troid Hastalık ve Böbrek Yetmezliği İle Seyreden Çöliyak Hastalığı Savas Öztürk1, Hatice Küçük2, Işın Kılıçaslan3, Emel Tatlı2, Fuat Sar2, Rumeyza Kazancıoğlu1 1Haseki Training and Research Hospital, Internal Medicine, Division of Nephrology, İstanbul Correspondence: Savas Ozturk, MD Address: Haseki Egitim ve Arastirma Hastanesi, Ic Hastaliklari, Nefroloji Servisi Haseki/Fatih/Istanbul/Turkey Tel: +902125294400/ 1709 Fax: +902123431000 E-mail: savasozturkdr@yahoo.com Received: 10.06.2009 Accepted: 23.11.2009 Code Number: gm10044 ABSTRACT Celiac disease (CD) may coexist with another autoimmune disorders. We presented a woman with coeliac disease coexistent with autoimmune hypothyroidism, nephrosclerosis and severe hyperparathyroidism. Forty years-old hypertensive woman, who had diarrhea without tenesmus, blood and mucus for 20 years, was admitted to hospital. Parathyroid hormone level was very high. Creatinine clearance was 44.5 ml/minute, and protein was 596mg/day. Renal biopsy revealed immunofluorescence negative chronic changes mimicking nephrosclerosis. The clinical and biochemical presentation of CD maybe complicated or differed from in renal failure patient. Especially management of serum phosphorus and PTH levels may have great importance. Key words: Celiac, autoimmune, hypothyroidism, nephrosclerosis, hyperparathyroidism. Çöliyak hastalığı (ÇH) başka otoimmün hastalıklarla birlikte olabilir. Burada, ÇH ile birlikte otoimmün hipotiroidizm, nefroskleroz ve ciddi hipoparatiroidizmin birlikte olduğu bir kadın hasta sunulmuştur. Kırk yaşında kadın hasta, 20 yıldır süren tenezmin eşlik etmediği, kansız, mukussuz ishal nedeniyle hastaneye yatırıldı. Parathormon düzeyi çok yüksek idi. Kreatinin klirensi 44.5ml/dakika, proteinüri 596mg/gün idi. Böbrek biyopsisinde, nefroskleroz ile uyumlu immunofloresan negatif kronik değişiklikler saptandı. ÇH’nin klinik ve biyoşimik bulguları, renal yetersizlikli hastalarda komplike veya farklı olabilir. Özellikle serum fosfor ve parathormon düzeylerinin yönetimi büyük öneme sahiptir. Anahtar kelimeler: Çöliyak, otoimmün, hipotiroidizm, nefroskleroz, hipoparatiroidizm INTRODUCTION Celiac disease (CD) is an illness causing malabsorption which is due to damage of the absorptive mucosa of the small intestine (1). CD may coexist with another autoimmune disorder. Herein we presented a woman with celiac disease coexistent with autoimmune hypothyroidism, nephrosclerosis and severe hyperparathyroidism. CASE Forty years-old woman admitted to the hospital with complains of dysuria and pollakuria which have been continuing for 4 months. Furthermore, she had diarrhea for 20 years. The diarrhea was bloodless and without tenesmus and mucus, frequency was 3-4 times in a day. She also had erythema induratum (erythematosus nodular lesion which has been diagnosed 4 months ago) in bilateral crural regions for 2 years and hypertension for 1 year. At physical examination: Skin was pale without edema. Thyroid gland was non-palpable. There were multiple eritemateus, brownish, nodular lesions with 5-20 mm diameter in at left elbow and bilateral crural regions. Arterial tension was 140/90 mmHg, pulse was 80/min, rhythmic. Other systemic examination was normal. Main laboratory analyses were shown in Table. In 24 hours urine analysis; creatinine clearance 44.5 ml/minute, protein 596 mg, calcium 14.28 mg/dl, phosphorus 6,7 mg/dl, magnesium 65 mg/dl, sodium 82 mEq/L, potassium 37 mEq/L, chlorine 92;8 mEq/L. In renal ultrasound, size of right kidney was 93.7*29.1 mm, and left kidney was 112.2*44.7 mm with increased bilateral echogenicity. Doppler ultrasound of renal arteries was normal. Kidney biopsy was done. In histopathological examination: 2 of 6 glomeruli were global sclerotic, other glomeruli showed mild hypertrophy, vascular capillaries and basal membranes were normal. In addition that focal tubular atrophy, widespread hyaline casts, mild interstitial chronic inflammation and mild fibrosis were demonstrated. Mild hyperplastic arteriolar changes were also determined (Figure). Immunofluorescence was negative for IgA, IgG, IgM, C3, fibrinogen and C1q in 10 glomeruli. These findings were accepted to be associated to nephrosclerosis. Furthermore, dual X-ray absorptiometer showed osteoporosis at L2-L4 vertebrae and spine (T score: -2.58 and -2.59, respectively). Thyroid and parathyroid glands ultrasound were normal, parathyroid scintigraphy did not show any adenoma. Duodenal biopsy revealed villus atrophy, crypt hyperplasia, lymphoplasmocytes and eosinophils-rich polymorphonuclear leukocyte infiltration. Anti-gliadin antibody IgA and IgG were negative but anti- endomysium antibody was positive. The patient was accepted as celiac disease and her diarrhea was recovered with gluten-free diet. On the other hand, thyroid stimulating hormone (TSH) was high, free T4 was at lower limit, anti-thyroid peroxidase was high, and therefore the patient was diagnosed autoimmune hypothyroidism and levothyroxine 100 mcg/a day was initiated. Gastrin, insulin, and C-peptide levels were within normal limits. Consequently the patient was diagnosed Hashimoto thyroiditis, celiac disease, nephrosclerosis related chronic renal insufficiency, and secondary hyperparathyroidism. Gluten-free diet and dietary restriction of phosphorus were initiated. Calcium including phosphorus binder, levothyroxine, oral iron supplementation, parenteral 25-hydroxy vitamin D, and diltiazem oral were also prescribed to the patient. DISCUSSION The primary findings of celiac disease are mucosal inflammation, crypt hyperplasia, and villous atrophy besides serological markers (1). Current evidence suggests that celiac disease is predominantly an immunologically mediated disorder involving an inappropriate T-cell mediated immune response to dietary gliadin (2). It may also coexist in patients presented with another autoimmune disorder. In the presented patient, the diagnosis of celiac disease has been made by intestinal biopsy which had typical histopathological findings. Intestinal malabsorption with impaired vitamin D absorption is frequently seen in celiac disease, like some other intestinal diseases. Moreover celiac disease is among the common causes of osteomalacia (3). In some patients with celiac disease, similar to our patient, gastrointestinal symptoms are not prominent and osteomalacia is the presenting feature (4). Vitamin D deficiency accounts for the vast majority of cases of osteomalacia. Patients with vitamin D deficiency, usually due to dietary deficiency or malabsorption, typically have hypophosphatemia, a low-normal to low plasma calcium concentration, low levels of calcidiol (25-hydroxy vitamin D), and evidence of secondary hyperparathyroidism (5). At presentation, our patient had very low serum 25-hydroxy vitamin D and hypocalcemia. However she had severe hyperphosphatemia and parathyroid hormone level was very high. The underlying renal impairment was blamed for high PTH level. Both impairment of excretion due to renal failure (despite high serum level, urinary phosphorus level was low) and bone resorption due to hyperparathyroidism were assumed to be responsible this high serum phosphorus level. Secondary and even tertiary hyperparathyroidism were reported in celiac disease. Additionally, seven cases of primary hyperparathyroidism due to sporadic adenoma occurring in a series of 310 patients (2.3%) with celiac disease have been demonstrated (6). In a study on secondary hyperparathyroid patients with control group conducted by Jorde R et al. 4 of 97 patients in hyperparathyroid group showed positive serologic test for CD whereas no case in the control group (7). Reduction in bone mass related to the presence of secondary hyperparathyroidism has been shown in gluten patients. In a similar study, Valdimarsson T et al. (8) showed that SHPT was found in 27% (28 of 105) of CD patients. In the same study, in patients with SHPT serum levels of 25-hydroxy vitamin D were lower and those of alkaline phosphatase higher than in patients with normal PTH, but ionized serum calcium did not differ between the two groups. BMD was more severely reduced in patients with SHPT. So, authors suggested that PTH should be measured when the diagnosis of coeliac disease was made, as an indicator of more serious intestinal disorder and complicating bone disease. Hyperparathyroidism in our patient was accepted to be secondary to renal function impairment and osteomalacia. Since, adenomas of any parathyroid glands were not detected in screening and responded to the treatment and hormone levels decreased. Although the association of IgA anti-gliadin antibodies and IgA glomerulonephritis has been reported; there are both cases and experimental reports showing glomerulonephritis, most of which were IgA nephropathy, in celiac disease (9). Our patient had mild proteinuria beside renal dysfunction but not hematuria. Nevertheless the biopsy did not show any primary glomerulonephritis or immun-mediated nephritis. The biopsy showed glomerulosclerosis with vascular hyperplastic changes mimicking hypertensive nephrosclerosis. The patient also has Hashimoto’s hypothyroidism which been diagnosed with autoimmune markers. Although the coexistence of CD with autoimmune thyroid diseases is well known, our patient may be assumed to have a polyglandular autoimmune syndrome (especially type 3 c). The data suggest that 25-hydroxy vitamin D is the treatment of choice for patients with vitamin D deficiency due to intestinal malabsorption. On the other hand, Molteni N et al. (10) showed that at diagnosis of CD, the patients frequently had intestinal calcium malabsorption, as demonstrated by strontium test, with an early renal compensatory mechanism. After gluten-free diet, normalization of calcium absorption and decrement of midmolecule parathyroid hormone suggested a normalization of mineral metabolism, although a positive effect on bone mineral density was not evident at that time. Moreover, bone mineral density in patients responsive to diet did not differ from that in healthy controls. Persistent villous atrophy is associated with low bone mineral density, underlining the importance of keeping to a proper diet. In the light of these data, we started a treatment including oral calcium supplementation and parenteral 25-hydroxy vitamin D in addition to dietary restriction of phosphorus. As a result, along with gluten-free diet serum calcium, phosphorus and parathormon levels showed improvement. Celiac disease may present without predominance of intestinal symptoms. The clinical and biochemical presentation maybe complicated or differed from in renal failure patient. Especially management of serum phosphorus and parathormon levels may have great importance. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10044t1.jpg] [gm10044f1.jpg] |
| |||||||||

{kind=link}
{kind=link}