 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
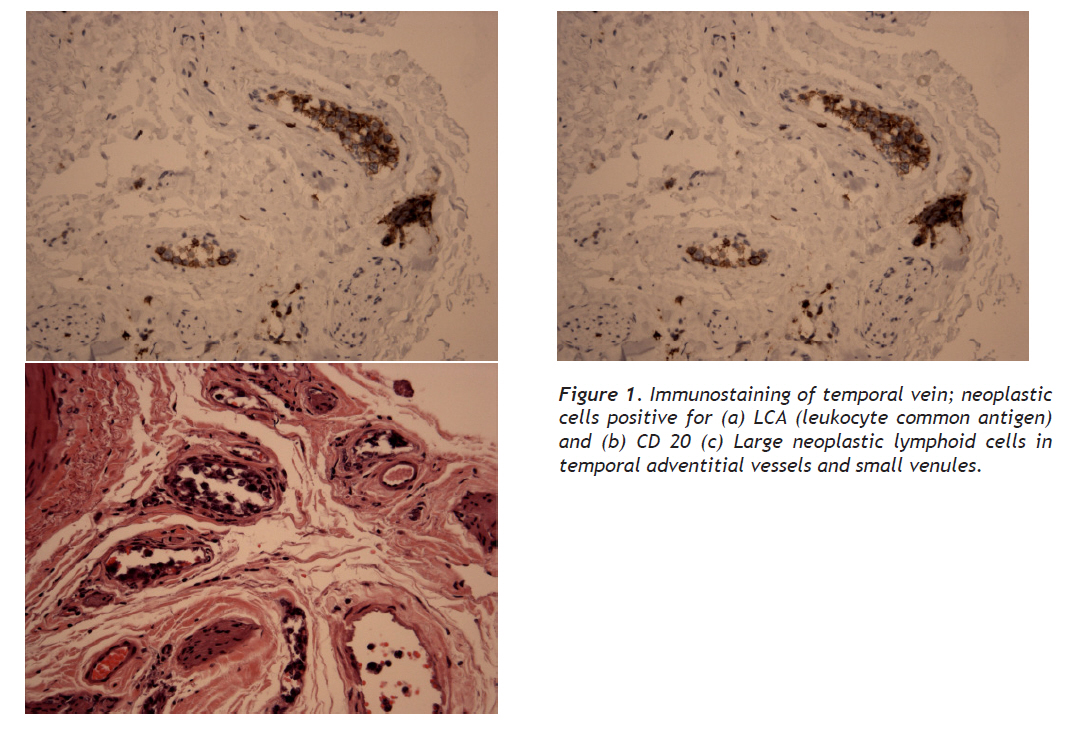
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 234-239 Case Report Angiotropic lymphoma: A Concealed Etiology of Fever of Unknown Origin Bilinmeyen Ateşin Gizli Bir Nedeni: Anjiotrofik Lenfoma Tabassum Nafsi1, Ming Valerie Lin1, John Stern2 Pennsylvania Hospital, Departments of Internal Medicine1 and infectious diseases2, Philadelphia, USA Correspondence: Tabassum Nafsi, MD, Department of Medicine, Pennsylvania Hospital, 800 Spruce Street, 1 Pine West, Philadelphia, PA 19107 Tel: (1) 215 829 3309 E-mail: tnafsi@yahoo.com Received: 04.03.2010 Accepted: 15.06.2010 Code Number: gm10045 ABSTRACT A 67 year old female presented with generalized weakness, falls and recurrent high grade fevers for 5 - 6 weeks. Physical findings included high grade temperature, lower extremity weakness and diminished reflexes. An extensive work-up for fever of unknown origin (FUO), including PET-FDG scan, did not yield any occult infectious or neoplastic process. Ultimately a temporal artery biopsy was planned to rule out temporal arteritis. The histopathology of temporal artery was normal while the vein showed lymphoid proliferation consistent with Angiotropic large cell lymphoma (ALCL). Key words: Fever Unknown Origin, lymphoma, PET scan 67 yaşında yaşlı bir kadın 5-6 haftadır süren ateş, halsizlik şikayetleri ile başvurdu. Fizik muayenesinde reflekslerinde azalma, alt ekstremitede zayıflık ve yüksek derecede ateş tespit edildi. Çekilen PET-FDG görüntülemesinde herhangi bir enfeksiyon ve maligniteye rastlanılmadı. Temporal arteritisi dışlamak için temporal arter biyopsisi alındı. Histopatolojisinde temporal arter normal iken vende anjiotrofik dev hücreli lenfoma tanısı konuldu. Anahtar kelimeler: Nedeni bilinmeyen ateş, lenfoma, PET BT INTRODUCTION Angiotropic large cell lymphoma (ALCL) is a rare malignancy with polymorphic clinical presentation and a high mortality rate if untreated. Owing to its non-specific presentation, cases often go unrecognized and ALCL is frequently a post-mortem diagnosis. Some cases of angiotropic lymphoma have been reported in the past few years with recent case reports demonstrating the utility of PET-FDG imaging as a diagnostic tool for ALCL presenting as fever of unknown origin (FUO) (1-4). We report a case of ALCL presenting as FUO. This case highlights that despite promising studies that normal PET scans have very high (95%) negative predictive value for infection and malignancy, ALCL presenting as FUO is still a challenging clinical diagnosis. Due to its occult presentation, tissue biopsy is necessary to diagnose and initiate appropriate therapy for this rare lymphoma. CASE A 67 year-old Asian female presents to the Emergency Department (ED) with worsening bilateral lower extremity weakness, lethargy and fever for six weeks. Six weeks prior to presentation, she developed high grade fevers, recurring daily; accompanied by chills and occasional cough with clear sputum. She was seen by her primary care physician and out-patient laboratory tests including blood cultures were negative. She was treated with Azithromycin for possible community acquired pneumonia for 2 weeks with no improvement in symptoms. Subsequently she noted generalized weakness and lower extremity weakness and 3 weeks prior to presentation, magnetic resonance imaging (MRI) of the brain and electromyography (EMG) were performed as out-patient and both were noncontributory. She was referred to an infectious disease specialist for further work up which included repeat blood cultures, urine culture, c-ANCA, p-ANCA and PET-FDG scan that were negative. Subsequently, she became debilitated with the progressive lower extremity weakness, had episodes of falls, lightheadedness and recurrent high grade fevers of 101oF. She was brought to the ED by her family. The review of systems was positive for decreased appetite, drowsiness and lethargy. She denied any rash, arthralgias, myalgias, headaches, visual symptoms, chest pain, abdominal or urinary complains. She has no significant past medical history. She is a retired Korean Pediatrician, living in United States for 30 years. She denied any smoking or alcohol history, and reported traveling to California 4 months before the onset of symptoms. On presentation to the ED, she was noted to have elevated temperature of 101 F, pulse rate of 110 beat per minute, blood pressure 98/51 and respiratory rate of 16 breaths per minutes. On physical examination, she was alert and oriented. She had muscle weakness and hypoactive deep tendon reflex in the lower extremities. There was no lymphadenopathy, chest was clear to auscultation; cardiac examination was unremarkable except for tachycardia. Abdominal exam was benign with absence of organomegaly. She subsequently became less responsive and arousable with a drop in her BP to 78/46 during examination. Admission labs showed: hemoglobin (Hgb) 9.2, hematocrit (Hct), 27.0, white blood cell count (WBC) 4.9, Platelet count 184; normal chemistry panel and Liver function tests (LFT), Albumin 2.9, INR 1.5 and erythrocyte sedimentation rate (ESR) 120. A chest radiograph showed left basilar opacity suggestive of pleural effusion or atelectasis, infiltrate could not be excluded. With high fever, hypotension and tachycardia as the presenting complain and a possible infiltrate on chest Xray; SIRS was the primary suspicion and she was pan-cultured, resuscitated with IV fluids and started on broad spectrum intravenous antibiotics. Computed tomography (CT) of thorax/abdomen/pelvis was negative except for incidental finding of uterine fibroids. Because of her ongoing symptoms of worsening fatigue, decreased appetite and hypotension and 6 week history of fevers; endocrine workup was done to rule out adrenal insufficiency. Endocrine workup was suggestive of central hypothyroidism and hypoadrenalism, with decreased levels of cortisol (6.3), ACTH (< 5), FSH (12.9), LH (8.9), growth hormone (2.6), free T3 (1.2) and T4 (4.1) with a positive ACTH stimulation test; prolactin (16.8) and TSH (0.57) were within normal limit. IGF-1 (insulin growth factor-1) was low at 41mg/dl. MRI of the brain revealed enlarged 3rd and lateral ventricles without transependymal flow which could be secondary to chronic long standing aqueductal stenosis. There was no acute ischemia or any pituitary findings of note. Our patient was placed on steroid and thyroid replacement therapy. She was also noted to have anemia that was consistent with anemia of chronic disease. During the course of the admission, the hemodynamic status and level of consciousness improved though our patient continued to have recurrent low grade fevers. Intravenous antibiotics were stopped on Day 3 after negative blood and urine cultures. Repeat CT scan of thorax and abdomen on day 5 showed relatively small, unremarkable adrenal glands, extensive subcutaneous edema and no other changes in comparison to previous study. Because of lower extremity weakness, EMG and lumbar puncture were done and both were inconclusive for any neurological or infectious cause. A subsequent MRI of the brain ruled out pituitary apoplexy. Differential Diagnosis: At this time, our patient met the criteria of FUO as described by Petersdorf and Beeson in 1961 (1). The workup for FUO includes a meticulous history and physical examination, complete hematological and serological workup, chest X-ray, multiple cultures and CT scan of abdomen and pelvis. The common causes of FUO are infections, malignancy and autoimmune process. We will focus on the most common cause of FUO; infectious disease. Our patient is of Asian origin, lives in New Jersey, traveled to California 4 months ago. She hails from an endemic area for Tuberculosis and volunteered a remote history of positive PPD. This was a new clue in the history though her Chest X-ray was negative. Extra-pulmonary tuberculosis has been noted to be the most frequent cause of FUO among systemic infections (1). There were no physical or radiological examination findings to suggest extra-pulmonary TB, nevertheless, given her persistent fevers, weight loss and night sweats, we could not ignore mycobacterial infections as a possible cause of her presentation. A bone marrow biopsy did not show any granulomatous disease. Nevertheless, empiric anti-tuberculous treatment (ATT) was commenced on day 9 and we continued to look for other causes of FUO. She was noted to have elevated lactate dehydrogenase (LDH) of 1255, with normal peripheral blood smear without evidence of malaria or babesiosis. Lyme titres were negative. Transthoracic echocardiogram and investigative workup for tick-borne diseases and systemic infections were all negative. The second most common cause of FUO is malignancy. History reveals decreased appetite and weight loss along with the fevers for 6 weeks. Our workup so far shows anemia of chronic disease, high LDH and ESR. A European study showed that the three parameters (anemia, high ESR and weight loss) had a low sensitivity (37, 52 and 46%. respectively), but a good specificity (92, 89 and 94 %. respectively) for malignancy (2). Our patient had a negative CT scan of thorax, abdomen and pelvis. A study by Bleeker- Rovers et al in 2003 concluded PET scans to be helpful tool in diagnoses of FUO with negative predictive value of 95% (3). PET with the glucose analogue 2-18F-fluoro-2-deoxy-D-glucose (FDG) is based on the enhanced glucose metabolism in neoplastic cells which identifies malignant process among the normal cells. PET scan has also been reported to have a high negative predictive value for the workup of malignancies and has been advocated as investigative tool for occult malignancies (3,4). Our patient had a negative PET scan. Bone marrow biopsy was also non-diagnostic of hematological malignances. The workup so far did not rule in or rule out any neoplasm. Autoimmune processes are the third common cause of FUO. Our patient has high ESR, normal C3, low C4, negative ANA and dsDNA. The most common rheumatologic causes of FUO with nonspecific serological findings are Giant cell arteritis and Adult Still’s disease. Our patient did not have any rash, arthralgias, myalgias or tenderness over temporal arteries; had high ESR and ferritin. As a diagnostic workup for FUO, temporal artery biopsy should be considered in the absence of headache or scalp tenderness (5, 7), so we consulted vascular surgery and an out-patient temporal artery biopsy was scheduled. During the course of admission, her vitals remained stable though she continued to have recurrent low grade fevers. She was discharged on day 10 on anti tuberculous medicines. She returned to the ED, 4 days after discharge with another episode of collapse followed by tonic-clonic movements for 20 – 30 seconds, high grade fever (103 F) and generalized weakness. At this point, all primary teams were re-consulted and temporal artery biopsy was performed. Diagnosis: During the procedure, the temporal vein was noted to be inflamed and both temporal artery and vein specimens were obtained for biopsy. Immuno-stain of temporal vein was positive for LCA (leukocyte common antigen) and CD20 and adventitial small vessels and venules showed large lymphoid cells consistent with Angiotropic Lymphoma (Figure 1). DISCUSSION Angiotropic Lymphoma is also known as intravascular lymphomatosis, malignant angioendotheliomatosis or angioendotheliomatosis proliferans. The disease was first described in 1959 by Pfelger and Tappeiner (6) as a proliferation of mononuclear cells within small vessels. As the name suggests, the cell of origin is thought to be endothelial. In 1985, Wrotnowski et al described the first case of malignant angioendotheliomatosis as angiotropic lymphoma (8) since the pathology is described as a lymphoid proliferation of small vessels. The more accepted term at present is Angiotropic Large cell Lymphoma (ALCL). ALCL is a rare malignancy with polymorphic clinical presentation and a high mortality rate if untreated. Owing to its non-specific presentation, cases often go unrecognized and ALCL is frequently a post-mortem diagnosis. Occlusion of vessels with lymphoid cells resulting in end organ ischemia, is the most common finding on autopsies and in addition to affecting CNS and skin, ALCL can present in liver (48%), lungs (73%), adrenals (67%), kidneys (79%) and heart (52%) (8). The clinical presentation of ALCL can be insidious and it can involve any organ system, though most common clinical findings are dermatological and neurological. Non-specific B symptoms like fever, night sweats and weight loss with a remarkable deterioration in performance status is the usual presenting feature of ALCL (9). Neurological features of ALCL are very variable and it can present non-specifically as dementia, change in mental status ranges from confusion, obtundance to coma, and focal neurological manifestation such as TIA, hemiparesis or paresthesias (10). Most case reports on autopsies have shown vascular occlusion in brain by tumor cells, probably causing the neurological signs (11). One third cases of ALCL have heterogeneous neurological symptoms at diagnosis (12). Neuro-imaging in ALCL is negative in half of the patients with neurological symptoms, though it should still be considered as a part of staging work-up of ALCL (12). Malignant cells in cereberospinal fluid (CSF) have been noted in advanced disease and a negative Lumbar Puncture should not rule out ALCL. Many cases of ALCL have been a post-mortem diagnosis but literature review reveals that fever (45%) has been a common feature in ALCL but was not recognized as such until recently. Fever associated with other B symptoms is seen in half of the cases while weight loss without fever has been seen in 10% cases. (18) ALCL presenting as FUO was first reported in 1999 by Kuvliev E et al (13). Most case reports of ALCL report fever and some other organ system involvement like pulmonary with hypoxemia or presentation similar to interstitial lung disease or renal involvement with proteinuria and renal failure. These presenting features are due to proliferation of vasculature by tumor cells; which has been noted on autopsies. Our patient presented with recurrent fevers and lower extremity weakness and the physical examination did not reveal any neurological cause for the weakness, and laboratory work-up was suggestive of central hypoadrenalism and hypothyroidism. Absence of other organ involvement and negative imaging studies made our case more challenging. The pituitary and adrenal gland involvement have been described in few case reports. Patients were found to have panhypopituitarism (7), hypoadrenalism (15,17) and SIADH (16) as part of the manifestation of this extra-nodal large cell lymphoma. Though, these cases had some identifiable lesion on imaging studies or were noted to have vascular proliferation of the involved organs on post-mortem examinations. Our patient presented with fever and panhypopituitarism but had no identifiable lesion on CT or MRI. Significant improvement in her symptoms was noted after steroid and thyroid replacement therapy was initiated though the fevers persisted until chemotherapy was started. At the writing of this report, the patient is receiving chemotherapy and is doing well. A study by Bleeker- Rovers et al in 2003 concluded PET-FDG scans to be a helpful tool in diagnoses of FUO and detection of occult inflammatory or neoplastic disease, both with a high negative predictive value (3, 18, 19). PET with the glucose analogue 2-18F-fluoro-2-deoxy-D-glucose (FDG) is based on the enhanced glucose metabolism in neoplastic cells which identifies malignant process among the normal cells. Despite recent case reports have describing the role of PET-FDG in detection of ALCL presenting as FUO (20), our patient had a negative PET scan and MRI brain showed finding suggestive of longstanding aqueductal stenosis but no identifiable lesion on the pituitary gland. Since PET scan was performed earlier on in our work-up for FUO, the negative result and its high negative predictive value kept malignant causes of FUO, lower in our differentials. In summary, ALCL is a rare B cell lymphoma, presenting mainly with systemic symptoms of fever, weight loss, night sweats, and cutaneous lesions with neurological symptoms. ALCL is an extra nodal B cell lymphoma proliferating in the blood vessels without any solid lesions; thus making it difficult to be detected by imaging studies. We report a case of ALCL that was a diagnostic challenge due its presentation as FUO, non specific serological markers, panhypopituitarism with negative pituitary, adrenal imaging and PET-FDG scan. This case is different from previously reported cases as our patient had atypical symptoms, did not have any identifiable lesion on imaging including negative PET-FDG scan and the diagnosis was derived solely from a temporal vein biopsy. We conclude that recurrent fevers and non-specific neurological signs such as asthenia and generalized weakness are not so rare in ALCL with a common laboratory finding of elevated LDH and ESR. It is important for physicians to remember ALCL as one of the differentials in FUO with non-specific systemic symptoms, and in the absence of negative imaging studies, tissue biopsy may be necessary for the diagnosis. A timely diagnosis of this fatal disease will allow the initiation of appropriate treatment and improve the clinical outcome. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10045f1.jpg] |
| |||||||||

{kind=link}