 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
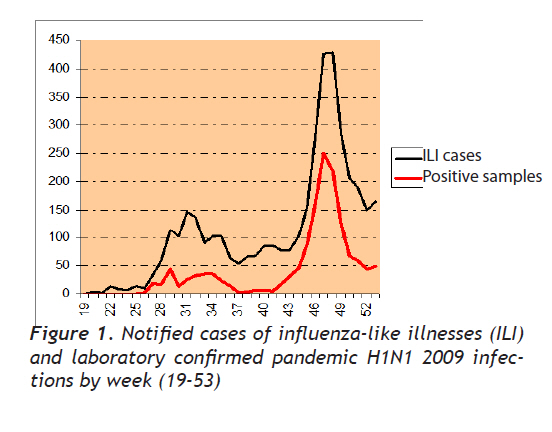
European Journal of General Medicine, Vol. 7, No. 2, April-June, 2010, pp. 240-244 Brief Report Epidemiological Surveillance of Pandemic H1N1 2009 infections in Northern Greece Kuzey Yunenistanda Pandemik H1N1 2009 Enfeksiyonun Epidemiyolojik Surveyansı G. Gioula1, M. Exindari1, A. Melidou1, D. Chatzidimitriou2, E. Chatzopoulou1, N. Malisiovas2 1National Influenza Centre for North Greece, Second Laboratory Department, Medical School, Aristotle University of Thessaloniki, Greece Correspondence: Dr Georgia Gioula, Lecturer of Microbiology B’ Microbiology Department, Medical School, Aristotle University of Thessaloniki Tel: +302310999121; fax: +302310999140, E-mail: ggioula@med.auth.gr Received: 05.03.2010 Accepted: 13.04.2010 Code Number: gm10047 ABSTRACT In response to the health emergency declared by the World Health Organization (WHO) in April 2009, Greece set up an enhanced surveillance system for pandemic H1N1 2009 by the 30th of April 2009. During the period of study (weeks 19-53), 3.903 suspected pharyngeal were examined at the National Influenza Centre for northern Greece. 1439 specimens were confirmed as pandemic H1N1 2009 (37.23%) infections. The hospitalization rate increased dramatically during November and December, while the death rate was 1.3%. Key words: H1N1, influenza, 2009, surveillance Dünya sağlık örgütünün 2009 yılının Nisan ayında bildirmiş olduğu acil durumda Yunanistan pandemik H1N1 2009 enfeksiyonu için surveyans sistemini geliştirdi. Çalışma dönemi içinde (19-53 hafta) 3903 şüpheli faringeali Ulusal Kuzey Yunanistan İnfluenza Merkezinde tarandı. 1439 örnek pandemik H1N1 2009 olarak tespit edildi (%37.23). Hastaneye yatma oranı Kasım ve Aralık ayında dramatik olarak artmıştır. Ölüm oranı %1.3 idi. Anahtar kelimeler: H1N1, influenza, 2009, surveyans The purpose of this study is to present information on the epidemiological characteristics of the cases of pandemic H1N1 2009 infections, reported in northern Greece, from April to December 2009 (weeks 19-53). During April 2009, a novel H1N1 virus was detected in epidemiologically unrelated cases of influenza-like illness in California and was subsequently recognized to be the cause of a major outbreak of respiratory disease in Mexico that had been already ongoing for some weeks. The virus was found to be an H1N1 virus that was antigenically and genetically unrelated to human seasonal influenza viruses and genetically related to viruses known to circulate in swine [1]. In response to the health emergency declared by the World Health Organization (WHO) in April 2009, Greece set up an enhanced surveillance system for pandemic H1N1 2009 by the 30th of April 2009. The main target was travellers returning from affected areas as well as their contacts. Thermal imaging cameras were installed at airports in order to detect incoming travellers with fever. A telephone hotline was used to provide information and guidance to the public, advise health professionals, and guide cases under investigation for pandemic H1N1 2009 to designated reference hospitals for clinical evaluation and nasopharyngeal swab collection. Specimens were sent to one of the two reference laboratories, in Athens (Hellenic Pasteur Institute) covering southern Greece and in Thessaloniki (Aristotle University of Thessaloniki, Second Microbiology Laboratory) covering northern Greece. In early July a third laboratory was introduced (University of Athens, School of Medicine, Department of Microbiology). All cases under investigation for pandemic H1N1 2009 were managed in the reference hospitals; they were referred there by primary care physicians, from non-reference hospitals, from other healthcare facilities such as airport medical offices, or they could present to the emergency department of a reference hospital on their own. This applied to both Greek and foreign citizens, regardless of insurance status [2]. Guidelines for case and contact management and for infection control were prepared by the Hellenic Centre for Disease Control and Prevention (HCIDC). These were sent to hospitals and published on the HCIDC website (http://www.keelpno.gr/articles/topic/?id=994). The case definition that was adopted in Greece, closely matches the case definition that was agreed upon on the European level [3]. A “case under investigation” was defined as an individual meeting the clinical criteria ie. fever >38oC plus symptoms of acute respiratory infection such as cough, dyspnoea, sore throat, etc. as well as the epidemiological criteria: history of travel to an affected area or history of close contact with a confirmed case during his/her infectious period. All cases investigated for pandemic H1N1 2009 were notified directly to HCIDC on an individual basis, both by hospital clinicians and by the reference laboratories. If the sample was PCR-positive for pandemic H1N1 2009 and the clinical manifestations were severe, the patients were hospitalized and specific treatment was administered. In the beginning of the outbreak, antiviral drugs were given to all suspected cases and their contacts. However, the following months antiviral drugs were given only to symptomatic high-risk groups. During the period of study (weeks 19-53), 3.903 suspected pharyngeal swabs and/or washes in 2SP (sucrose-phosphate) medium were examined at the National Influenza Centre for northern Greece. All specimens were accompanied by a Standard Form with information on age, sex, date of onset, date of specimen collection, place of residence, clinical features of each patient, travel history, vaccination history and administration of antiviral treatment. RNA was extracted with the Qiagen Viral RNA mini kit, according to the manufacturer’s instruction and pandemic H1N1 2009 infections were confirmed using the CDC swine influenza real-time RT-PCR kit, following WHO recommendations. A “confirmed case” was defined as a person tested positive for pandemic H1N1 2009. Results were reported to HCIDC, WHO and ECDC. On 27 May, the first pandemic H1N1 2009 infection was detected at a 20-year old student returning from the United Kingdom [4]. Between April and December 2009, 1439 specimens were confirmed as pandemic H1N1 2009 infections (37.23%). The age distribution showed a trend towards young adults, as the median age of cases was 27 years, ranging from 1 to 81 years old. Sex distribution showed similar infection rates at both sexes (52% men and 48% female). The analysis of these cases showed that after some sporadic cases and a slow increase in June 2009, a significant increase of newly reported cases was observed at mid July. During this first wave, the majority of the infected individuals (70%) were travellers. A second peak followed, that initiated at week 44 and lasted until the end of 2009. Opposingly, at this remaining period of study, September to December, only 35 patients were travelers. Since the beginning of January, there seems to be a downward trend in Greece (Figure 1). All confirmed cases were presented with ILI, with fever ranging from 38-40,5°C, acute onset of symptoms, cough, catarrh, sore throat, fatigue, headache, muscle pain and in some cases conjunctivitis, diarrhoea and/or vomiting. Among these cases, 210 (14,4%) have been hospitalized. The majority of them (192) were during the months November and December. The medical complications related to hospitalization were acute respiratory failure, pneumonia, hypoxia, acute tracheitis, and tracheobronchitis. A wide age range distribution was observed in hospitalized patients, but more severe outcomes were generally associated with older patients (median age 52 years old). Of the 1439 confirmed cases, 69 (4,7%) patients developed pneumonia, while 13 of them (1%) required admission to an intensive care unit. Twenty confirmed cases of pandemic H1N1 2009 infection resulted in death (1,3%). The median age of those patients was 47,4 years, ranging from 6 to 81 years old, while 13 out of 20 were male. No pandemic H1N1 2009-related deaths have been reported in pregnant women, while two pregnancies were spontaneously aborted at the third trimester, due to the infection. Obesity has been considered as a possible risk factor of the fatal cases. This condition was found in 2 of the fatal cases. Additionally, 9 of the above patients had an underlying condition, while four of them were completely healthy before the infection. There were also a small number of asymptomatic cases, mostly detected during the summer period. Regarding the antiviral treatment, at the onset of the pandemic, all patients received oseltamivir (Tamiflu) after the confirmation of pandemic H1N1 2009 infection, but only 21% of the cases were treated from the onset of the symptoms. After widespread transmission within the country, patients no longer received antiviral treatment unless necessary. During the period September to December, only 75 confirmed cases received antiviral treatment (5,2%). The information on the vaccination status for seasonal influenza was requested at the patient’s standard form. 85 patients (5,8%) were vaccinated for seasonal influenza (2009-2010 season), the majority of the vaccinations (83 out of 85) occurred during November. 10 patients reported vaccination for the previous season, 2008-2009. It is worth mentioning that 3 of the confirmed pandemic H1N1 2009 cases have been vaccinated with the vaccine that contained the pandemic strain. The results provide an overview of the epidemiological characteristics of 1439 infections by pandemic H1N1 2009, in northern Greece, between April to December 2009. The age distribution of the infections clearly indicates that the rate of infection is greater in the age group of 15-25 years old. The very low incidence of infections at individuals over 60 years of age is consistent with studies from other countries [5,6]. It is still unclear if this is due to a partial immunity from former infections with H1N1 influenza viruses or because the virus has not yet been sufficiently introduced in this subpopulation. Sex distribution, on the other hand, showed similar infection rates at both sexes, which seems to be similar to reports from other countries [7]. Additionally, the analysis of these cases showed that after some sporadic cases and a slow increase in June 2009, a significant increase of newly reported cases was observed at mid July. This trend was also reported from other countries in Europe [8]. A second peak followed, that initiated at week 44 and lasted until the end of 2009. Since the beginning of January, there seems to be a downward trend in Greece. It is notable that there has been recently a change in health-seeking behaviour. The first anxiety about the new infection clearly has forced more people suffering from respiratory symptoms to seek medical assistance and therefore might have brought a vast number of cases to the attention of the public health authorities. Our data show that most common symptoms include fever, cough, catarrh, sore throat, fatigue, headache and muscle pain, which means that most cases of pandemic H1N1 2009 currently seem to have mild, uncomplicated clinical features. This agrees with reports from other countries [9,10]. Asymptomatic patients were mostly detected during the summer period, during which all contacts of laboratory confirmed cases were investigated. After widespread transmission of the virus within the country, clinicians had to address possible cases only if cough, high fever or more severe symptoms were present. It is also remarkable that the hospitalization rate changed considerably over the weeks. During the first weeks, the majority of cases were hospitalized due to infection control measures. Even though that might still be the case for some patients, hospitalization is now considered as a proxy for the severity of the disease in patients. A closer look at those cases shows that patients with underlying conditions had two times higher hospitalization rate than in cases without underlying conditions, while more severe outcomes during hospitalization were generally associated with older patients. This is similar to findings from other countries as well [7]. It is also important to note that some hospitalizations were due to isolation purposes or due to underlying medical conditions and therefore the proportion to patients admitted to hospital is not an indicator of the severity of the disease. According to our results the death rate was 1,3%, similar to the percentage worldwide (1,2-1,3%), though the mortality in Europe had not been reported higher than 0,44% (http://www.who.int/csr/disease/swineflu/en/). Regarding this relatively high case-fatality ratio, it should be considered that only the laboratory-confirmed cases were accounted. In the beginning of the pandemic in Greece, antiviral treatment was administered to all patients after laboratory confirmation of the infection. According to reports from other countries, all patients received antiviral treatment especially at the onset of the pandemic as well [11]. This policy was soon abandoned due to the high risk of development of resistant pandemic H1N1 2009 strains. Furthermore, antiviral susceptibility tests are considered essential to monitor possible spread of resistant strains within the population. On the other hand, in a study conducted in Italy, the number of individuals reported to have been vaccinated during the 2007-8 and 2008-9 seasons was 9 and 2 out of 73 respectively [11]. All similar studies, on international level, support the importance of surveillance activities in order to monitor the pandemic and guide public health actions by collecting data on epidemiological parameters and mechanisms of virus transmission in the community. Acknowledgements The authors would like to thank the Hellenic Centre for Disease Control and Prevention (HCIDC) for their contribution to the pandemic H1N1 2009 surveillance and also for the enormous volume of work undertaken by them. REFERENCES
Copyright 2010 - European Journal of General Medicine The following images related to this document are available:Photo images[gm10047f1.jpg] |
| |||||||||

{kind=link}