 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Human Genetics, Vol. 8, No. 1, Jan-Jun, 2002 pp. 20-25 Spermatogenic Alterations in Men with High Testiculo Epididymal Temperatures
Rima Dada1, NP Gupta2, K Kucheria3 Department of Anatomy1
and Urology2, All India Institute of Medical Sciences, New Delhi-110029,
India. Code Number: hg02005 Sperms are produced by a highly complex and poorly understood differentiation process known as spermatogenesis. Occupational exposure to high temperatures adversely affect testicular function causing partial or complete spermatogenic arrest. Dyers, cooks, blast furnace workers and men with varicocele are known to develop testicular hyperthermia, which leads to oligoasthenoteratozoospermia (OAT) and azoospermia. Semen analysis of 125 infertile men (and 25 fertile controls following the WHO guidelines, 1999 showed azoospermia in 109 men and oligozoospermia in 16 men. Twenty azoospermic and 14 oligozoospermic men had high testiculoepididymal temperatures either due to occupational exposure to high temperature or varicocele. All the 14 oligozoospermic men showed a very high percentage of sperms with abnormal morphology, impaired motility and they were subclassified as OAT group. Observations made in this study reiterates that high intratesticular temperature causes partial or complete spermatogenic arrest and may lead to increased production of morphologically abnormal sperms with impaired motility. This inverse relationship of sperm function with elevated temperature has implications in clinical medicine both in understanding pathological states and for therapeutic measures. Key words: Spermatogenic arrest, Oligoasthenoterat-ozoospermia, azoospermia, Hyperthermia, Oligozoos-permia, semen. About thirty to forty percent of men in the reproductive age group have qualitative or quantitative defect in sperm production. Sperms are produced by a highly complex process of spermatogenesis. Any partial or complete disruption of this process results in spermatogenic arrest and finally leads to oligozoospermia and azoospermia respectively. In oligozoospermia the sperm concentration is less than 20 million/ml and in azoospermia there is complete absence of sperms in the semen. For normal fertility a man requires normal spermato genesis, successful epididymal storage and normal sperm transport. Based on these functions the causes of infertility can be secretary or excretory. Secretary cause is due to spermatogenic arrest while in excretory cause spermatogenesis is normal but there is obstruction to the outflow of spermatozoa. Besides this the fertility in males depends on normal linear progressive sperm motility and normal sperm morphology. Sperm motility is the best predictor of fertility potential in man. Several conditions like exposure to high temperature, certain pesticides, drugs and deletions of Azoospermia Factor loci (AZFd), varicocele can affect sperm production and motility adversely. The normal human sperm measures 50-60 ìm in length and has head, neck, middle piece and tail. The head is oval in shape whereas midpiece is slender, straight, regular in outline and is aligned with the long axis of the head. Its width is about one third of the head. The tail is slender, straight and regular in outline. Normally testicular temperature is maintained 2-3°C lower than the core body temperature and is an important prerequisite for efficient spermatogenesis as germ cells and sustentacular Sertoli cells are highly sensitive to hyperthermia. Various occupational factors and environmental agents have been shown to have deleterious effect on male reproductive function and it is difficult to elucidate the role of a single agent. Several confounding factors related to diet, life style, stress and socioeconomic status also affect semen quality. Though reports are available regarding the effects of hyperthermia on semen quality but very few of these highlight the effect of high temperature on sperm morphology. The present paper reports spermatogenic arrest leading to low sperm counts and increased number of morphologically abnormal sperms with impaired motility in males with high testiculoepididymal temperatures.
Materials and Methods
One hundred and twenty five infertile males who were diagnosed as infertile at Urology Clinic of All India Institute of Medical Sciences, New Delhi were included for this study. Couples are said to be infertile if the wife is unable to concieve after 1 year of regular unprotected intercourse. Twentyfive fertile men whose wives had conceived within 1 year of marriage were controls (control group). Information was recorded from patients and controls about their occupation, type of work performed, period of cohabitation, any recent illness, medication taken, exposure to irradiation, consumption of alcohol, smoking, eating habits, use of recreational drugs and family history in a predesigned performa. Cytogenetic and Molecular analysis was performed according to guidelines prescribed by Simoni et al. (1999). Detailed general physical examination was performed for each patient. FSH and LH levels were assessed for each patient to determine the testicular damage and to confirm that the cause of infertility was secretary. A minimum of 2 semen samples were collected at an interval of 1 month from each patient. Semen samples were allowed to liquefy at room temperature and seminal volume, pH, sperm count, motility and morphology were analyzed within one hour of collection using WHO guidelines, 1999. For assessing the sperm motility the microscope field was examined and motility of each spermatozoa was classified as A (rapid linear progressive motility), B (slow or sluggish linear or non linear motility), C (non progressive motility) and D (immotile). For studying the sperm morphology a drop of semen was smeared on a clean glass slide. The smear was then air dried and fixed in a mixture of equal parts of ethanol and ether. The slides were then stained with 2% Giemsa stain for 30 minutes. Stained slides were analysed under oil immersion x100 objective to assess for morphological abnormalities of sperm head, midpiece and tail. A total of 100 sperms per sample were scanned to count and classify sperms with abnormal morphology such as small, pin, large amorphous, tapered, double and triple head; dilated or bent midpiece and coiled or short thick tail. The mean and standard deviation were calculated using standard statistical methods and t test to study the significance from two samples assuming unequal variances.
Results
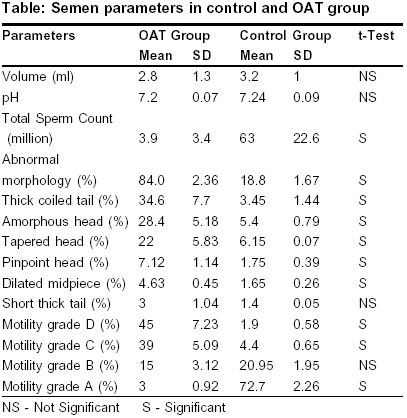
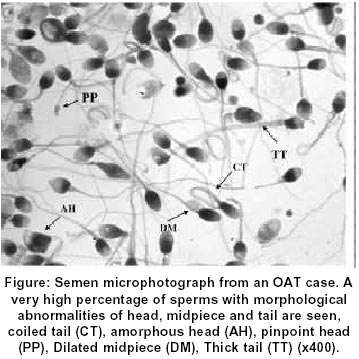
Semen analysis was done in 125 infertile males and 25 controls. Mean age of the patients was 28.3 years (17-53years) and the mean duration of marriage was 6 years (1-30 years). Of the 125 infertile males, 109 males had no sperms in their ejaculate and were classified as azoospermic. Sixteen males had a total sperm count less than 20 million sperms and were classified as oligozoospermic. In two of the 16 oligozoospermic males the total mean sperm count was 6.25 million with more than 75% of the sperm showing normal morphology. The mean seminal volume was 4±1.8 ml and the mean pH was 7.2±0.08. These sperms had oval head with acrosomal cap covering more than one third of the head surface. The midpiece was cylindrical in shape and its width was less than one third the width of the head. The tails were long, slender and straight. About 20% sperms showed abnormal morphology. Remaining 14 oligozoospermic males were found to have a very high percentage of morphologically abnormal sperms with impaired motility a picture characteristic of OAT and formed OAT group. These OAT cases were analyzed in detail and results were compared with control group (Table 1). Semen volume and pH in OAT group were slightly lower than the control group, which was not significant (p>0.05). The average total sperm count in OAT group was 3.9 million which was significantly (p<0.05) lower than the control group. The mean percentage of sperms with morphological abnormalities (Figure1) such as thick coiled tail, amorphous head, tapered head, double head and dilated midpiece were significantly higher in OAT group as compared to the control group (p<0.05). The mean percentage of sperms with motility grade C and D were significantly higher in OAT group than in the control group (p<0.05) and motility grade A was significantly lower than the control group (p<0.05).The mean percentage of sperms with motility grade B was lower than the control group which was not significant (p>0.05). The mean FSH and LH levels (17.07+1.8 mIu/ml and 24±1 mIu/ml) were significantly higher (p<0.05) in the OAT group males as compared to the control group (3.54 ±0.29 mIu/ml and 6.4± 0.1 mIu/ml). Correlation With Aetiological Factors In 20 azoospermic and 14 males with OAT, there was one common underlying aetiological factor. Of these 34 men, twenty four men had been exposed to very high temperature at their work place for a period of 5-15 years. They were working in blast furnace (n=6), Cement, brick, glass and plywood preparation factory (n=6), melting tar (n=7), Dyers (n=4), Welder (n=1). The rest of the ten men had varicocele, a condition in which the pampiniform plexus of veins are dilated and are associated with raised testicular temperature. Varicocele and occupational exposure to consistently high environmental temperatures may have led to increased intratesticular temperatures in these men. There was no significant history of smoking, medication, viral illness or use of any recreational drugs in these males. Rest of the 86 azoospermic and 2 oligozoospermic males had associated history of infections, cryptorchidism, mumps, iatrogenic factors which may have some role in developing complete or partial spermatogenic arrest, thereby resulting in azoospermia and oligozoospermia. Of these, 29 males had numerical and structural chromosomal aberration and in 8 cases there were Yq microdeletions, details of these findings have been discussed elsewhere.
Discussion
Scrotal temperature is maintained 2- 3°C lower than the body temperature and this is an important prerequisite for optimal spermatogenesis. The germ cells and Sertoli cells are highly sensitive to elevated temperature which causes partial or complete spermatogenic arrest (Martin du Pan and Campana, 1993). Previous studies have shown that some men have intrinsic defect in scrotal thermoregulation and about 80% of men with oligozoospermia have elevated scrotal temperatures (Zorgniotti and Sealfon, 1988). Even in normal fertile males fever, high summer temperatures and frequent hot baths, saunas are known to result in destruction of germinal epithelium and also induces transient oligozoospermia (Bedford1991, Mieusset et al.1991). Bedford in 1991 proposed that cauda epididymis is sensitive to high temperature. High scrotal temperature causes rapid disruption of absorptive and secretory function of cauda epithelium thereby changing protein composition of cauda fluid and causing reduction of its storage capacity. In present study 24 infertile males had exposure to high temperature at their work place for a mean period of 8.5 years and 10 men had varicocele a condition associated with high testiculo-epididymal temperatures. It is possible that in these men exposure of testes to high occupational environmental temperature led to an elevation of intratesticular temperature as in men with varicocele. This elevation of intratesticular temperature may have led to spermatogenic arrest and led to production of morphologically abnormal sperms with impaired motility to complete absence of sperms in the semen. Dyers, welders, cooks, steel and blast furnace workers are exposed to high temperatures at their workplace and are reported to have impaired spermatogenesis (Tas et al, 1996, Setchell, 1998). Thus testicular hyperthermia has been postulated to lead to spermatogenic arrest. Available literature suggests that short term exposure to high temperature may cause reversible changes in the seminiferous tubules whereas chronic exposure leads to irreversible damage to the seminiferous tubules. In the present study it was observed that men exposed to high temperatures for 5-7 years had OAT while those exposed for 12-15 years had azoospermia. Thus it seems that with increased duration of testicular hyperthermia the severity of spermatogenic arrest increases. Ten men had varicocele a condition known to cause decline in semen quality by raising the testicular temperature and is found in about 15% of the general population (Belloli et al, 1993). Thirty five percent of men with primary infertility (range: 19%-41%), and in 80% of men with secondary infertility have varicocele (Pyror and Howards 1987). Improvements in sperm motility, morphology, testicular size and testicular histology have been observed after varicocelectomy, thus resulting in initiation of pregnancy in 50%-80% of cases (Krause 1998). There are several hypotheses to explain the mechanisms by which varicocele may exert a deleterious effect on spermatogenesis and fertility. These include renal and adrenal reflux, hypoxia, hormonal dysfunction, and hyperthermia. The most widely accepted view to explain the deleterious effect of varicocele on spermatogenesis is that of raised testiculoepididymal temperature. In the present study no surgical correction was done for the seven azoospermic and three oligoasthenoteratozoospermic men with varicocele. This might have led to a gradual decline in semen quality leading to OAT and then azoospermia. Maturation arrest at primary spermatocyte phase and at spermatid stage is observed in men with varicocele (Mcfadden and Mehran, 1978, Spera et al, 1979). Zini et al.2000 reported that varicocele is a progressive condition that can result in infertility in cases with previously established fertility. Varicocele is associated with abnormal sperm morphology, increased production of reactive oxygen species (ROS) and thus defective sperm function. Wang et al. 1997 reported that elevation of testicular temperature by 1°C above the baseline depresses spermatogenesis by 14% and thus decreases sperm output. Exposure to high temperature also results in modification of sperm morphology. It is characterized by increase in the number of morphologically abnormal sperms. The mean value of sperms with abnormal morphology rises from 30 to 60% within 6-8 months of exposure to high temperature (Wang et al, 1997). They postulated that heating the testes induces a depression not only in the amount but also in the quality of sperm output. Though a number of studies have reported about deterioration in semen quality on exposure to high temperature and elevated testicular temperature but to the best of our knowledge very few studies have reported about the increase in specific morphological abnormalities of sperms. In our study we found that 84% sperms had abnormal morphology. The most predominant abnormality was thick coiled tail (34.6%), amorphous head (28.4%), and tapered head (22%). Though percentage of sperms with morphological abnormalities rises sharply within 6-8 months of raised testicular temperature (Mieusset and Bujan 1994, Levine et al, 1992). In the present study the cases had exposure for a mean period of 8.5 years. Wang et al. 1997 explained that elevated testiculo-epididymal temperatures decreases the synthesis of sperm membrane coating protein which in turn results in the production of morphologically abnormal sperms. Only 3% sperms showed linear progressive motility and whereas majority (84%) of sperms had impaired motility (grade C and D). Increase in number of morphologically abnormal sperms results in impaired motility as normal intact sperm morphology is prerequisite for linear progressive motility. Gandini et al. 2000 postulated that sperm function is strictly correlated with sperm morphology and that sperm motility is the best predictor of fertility potential in man. Functional and fully differentiated Sertoli cells are critical for development of quantitatively and qualitatively normal spermatogenesis. They also provide structural and functional support to the developing and differentiating germ cells as each Sertoli cell is in contact with 47 germ cells and 5 other Sertoli cells (Orth et al, 1988). High testicular temperature damages the Sertoli cells and their number decreases impairing spermatogenesis. This leads to a decrease in the number of germ cells with incomplete differentiation (Steger et al, 1999). Damaged Sertoli cells produce decreased amount of inhibin which decreases negative feedback on pituitary leading to increase in FSH level. This increase in FSH level is directly proportional to the Sertoli cell damage that indicates the severity of testicular damage. FSH levels are the most important endocrine parameter to evaluate testicular function (Bergmann et al, 1985). FSH and LH levels were elevated in azoospermia and in OAT cases. The difference in FSH and LH levels between OAT group and control group were statistically significant (p<0.05). One of the well known mechanism to explain spermatogenic impairment due to hyperthermia is activation of p53, a tumour suppressor gene which is expressed in testes (Rogel et al, 1985, Almon et al, 1993). Its level of expression is highest in pachytene spermatocytes (Schwartz et al, 1993). High scrotal temperatures cause condensation of nuclear chromatin which causes p53 activation which leads to cell cycle arrest. This prevents clonal proliferation of germ cells with damaged DNA. Morgentaler et al. (1999) postulated that p53 might play a role in heat induced germ cell apoptosis. p53 is located on the nuclear membrane in the normal germ cells and is involved in quality control of germ cells. It translocates to the nucleoplasm with heat induced nuclear damage and induces germ cell apoptosis (Yin et al, 1997). In the past decade, male reproductive health has declined with marked increase in the population of subfertile males (Carlsen et al, 1992). The sperm count has been falling at an alarming rate of 2% per annum for the last 20 years. This is believed to be due to increase in global temperature and environmental pollution. There has been an yearly decline of 2.6%, 0.3% and 0.7% in sperm concentration, sperms with normal motility and sperms with normal morphology (Tas et al, 1996). Thus, the testes is remarkable as a biological system for its functional regulation by temperature. The testes function optimally at relatively cool temperature and high testicular temperatures impair spermatogenesis leading to OAT and azoospermia as has been seen in the present study. Observed temperature sensitivity of testes has implications in clinical medicine both in understanding pathological state and for therapeutic measures. The results of this preliminary study show that in men with raised testiculoepididymal temperatures either due to varicocele or occupational exposure leads to spermatogenic arrest which leads to oligoasthenoteratozoospermia and azoospermia.
Acknowledgements
This work was supported by Indian Council of Medical research (ICMR).
References
Copyright 2002 - the Indian Society of Human Genetics The following images related to this document are available:Photo images[hg02005t1.jpg] [hg02005f1.jpg] |
| |||||||||

{kind=link}
{kind=link}