 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Human Genetics, Vol. 8, No. 2, Jul-Dec, 2002 pp. 45-51 Review Article The Impact of Consanguinity on the Indian Population A. H. Bittles Centre for Human Genetics, Edith Cowan University, Perth, Australia.
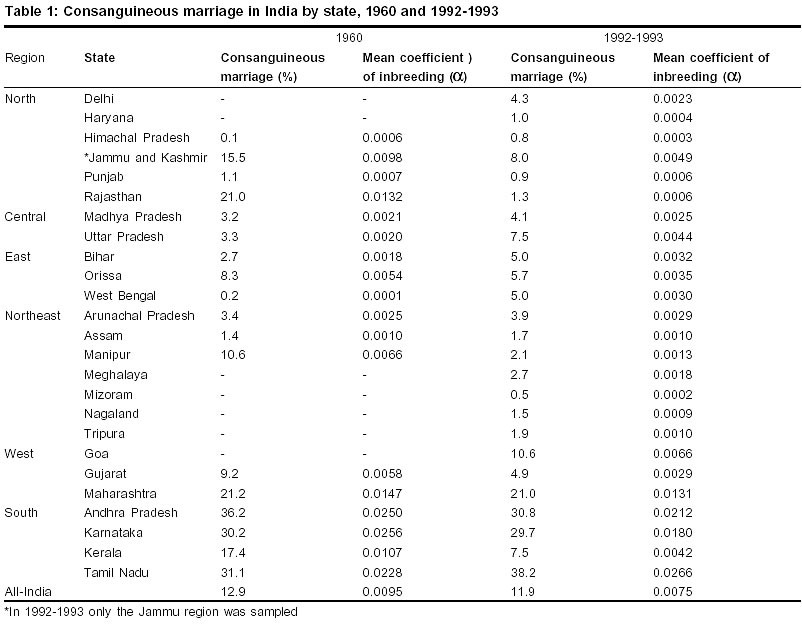
Code Number: hg02010 Numerous studies have been conducted by Indian anthropologists into the prevalence of both consanguineous and affinal marriage.1-3 and the topic of consanguinity continues to attract great attention among geneticists and social scientists. The strengthening of family relationships is of primary importance in the preference for close kin unions, with economic benefits an additional consideration. Consanguinity does not appear to adversely affect human fertility. However, both postnatal morbidity and mortality are increased, with greatest effect so far observed in the early years of life. With declining mortality and morbidity due to infectious disease, recessive genetic disorders will progressively gain greater prominence in the overall spectrum of ill-health. This change will be especially obvious in communities which practise consanguineous marriage, and in small highly endogamous communities where random drift occurs. Key words: Consanguineous marriage, endogamy, drift, recessive disorders, India Introduction The population of India is unique in its size and in the level of sub-division, with 15 major languages and six main religions. Within the majority Hindu community there are an estimated 3,000 major castes, 1,055 scheduled castes and 572 schedules tribes.4 The Muslim population of over 130 million is similarly sub-divided into Sunni, Shia, Ismaili and Dawoodi Bohra communities, and biraderis that are based on traditional social and occupational divisions. The net result is that the national population of over 1,000 million comprises some 50,000 to 60,000 endogamous sub-populations.5 The profound influence of caste endogamy has been confirmed by genomic analysis of modern Indian populations which has confirmed the continuing high level of gene differentiation,6 with marked divisions according to caste rank.7 While caste endogamy is universal, India is sub-divided into two major regions with respect to a preference for, or avoidance of, consanguineous marriage. The mainly Indo-European speaking Hindu peoples in the northern states avoid marital unions between biological kin, because of a prohibition on consanguineous marriage believed to date back to approximately 200 BC.8,9 By comparison, there is a long tradition of uncle-niece marriage and unions between a man and his maternal uncle's daughter (mother's brother's daughter) in South India.10 Consanguineous marriage is common in all Indian Muslim communities.11 Variations are, however, seen in the levels of consanguineous unions contracted in different branches of Islam and between specific communities, and these differences emphasize the important influence of local and regional customs in the arrangement of marriage contracts. The overall effects of these various influences are illustrated in Table 1 which lists the prevalence of consanguineous marriage reported in a survey based on 587 villages, conducted alongside the 1961 Census on the advice of JBS Haldane.1 In some cases the state numbers sampled were small and and/or unrepresentative, e.g. Rajasthan in which just four villages and a total of 442 couples were investigated, and Manipur where only Christians were sampled. By comparison, the 1992-1993 National Family Health Survey (NFHS) was planned and undertaken as a nationally representative survey.12 Overall, there was only a modest change in the national level of consanguineous marriage reported, from 12.9% in 1961 to 11.9% in 1992-1993. In some cases the data were quite discrepant, e.g. Gujarat, Manipur, Rajasthan and Uttar Pradesh, which again was probably due to the uneven sampling format of the earlier survey, but in both surveys the highest rates of consanguineous marriage were reported in Andhra Pradesh, Karnataka and Tamil Nadu. The data suggest some decline in the popularity of consanguineous marriage in these three states. The differences observed may, however, mainly be associated with the different sampling regimes employed. The 1960 survey was conducted only in villages whereas the 1992-1993 NFHS collected data from both urban and rural respondents, and in all surveys in South India consanguineous marriage has been shown to be significantly more common in rural areas.13 The decline in consanguineous marriage in Kerala does, however, appear to be genuine. The genetic effects of consanguineous marriage For most purposes a marriage is regarded as consanguineous if it has been contracted between spouses who are related as second cousins or closer (F = 0.0156), since the levels of homozygosity in marriages beyond second cousin (F <0.0156) differ only to a minor degree from those observed in the general population. As indicated in Table 1, at the population level the mean level of inbreeding (a) can be calculated according to the formula: a = SpiFi where S is the sum of the proportion of individuals pi in each consanguinity category Fi. Composite figures for different Indian communities and other non-Indian populations have been compiled14 and also are available at the website http://www.consang.net. In many well-established communities in South India there is a long and apparently unbroken history of consanguineous unions. Under these circumstances the cumulative level of inbreeding may be significantly higher than the value calculated for a single generation. A correction can be applied to account for the effects of ancestral inbreeding using the formula: F = å (½)n (1 + FA) where FA is the ancestor's inbreeding coefficient, n is the number of individuals in the path connecting the parents of the individual, and the summation (å) is taken over each path in the pedigree that goes through a common ancestor. For a large majority of clinical studies only the effects of consanguinity in the current generation are considered. As indicated above this may underestimate the actual level of homozygosity in an individual. However, this decision is taken largely on practical grounds as in many communities where consanguinity is preferential the family pedigrees show complex pathways of inbreeding that are difficult and very time-consuming to interpret.
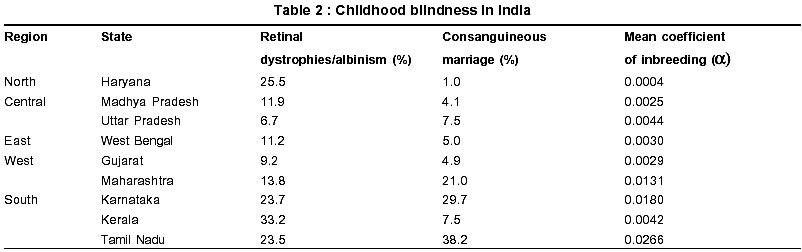
The influence of consanguinity on reproduction An overall assessment of the genetic influence on fertility within consanguineous unions is difficult, as information on early prenatal losses are usually dependent on maternal recall and the outcomes may be dependent on non-genetic factors, such as maternal age, birth order and birth interval.15 Enhanced genetic compatibility would be expected between mother and fetus in consanguineous unions, resulting in an advantageous pregnancy outcome because of decreased rates of ABO incompatibility16, and the clinically more severe Rh incompatibility17 and pre-eclamptic toxaemia.18 Conversely, according to the fetal allograft concept a balanced polymorphism for transplantation antigens may be maintained in mammalian species by a selective mechanism in which antigenic disparity between the mother and fetus is beneficial to fetal development.19,20 A comparative analysis of fertility in consanguineous and non-consanguineous marriages has been conducted, based on 30 populations and including 11 studies from India.15 At all levels of consanguinity investigated, from F = 0.0156 to 0.125, the mean number of live births was higher in the consanguineous unions when compared with marriages between non-consanguineous couples, and in the case of first cousin marriages (F = 0.0625) fertility was greater in 27 of the 30 populations investigated (p<0.0001). To some extent the higher fertility among consanguineous couples may be due to their earlier age at marriage and first successful pregnancy,21 and there also is evidence of reproductive compensation, i.e. with children who die at an early age rapidly replaced.15 Consanguinity-associated mortality Most studies in India have shown that early postnatal mortality is higher in the progeny of consanguineous unions, due at least in part to the expression of deleterious recessive genes. Consanguinity-associated deaths are largely concentrated during the first year of life,22 and multiple deaths have been reported in specific consanguineous families in proportion to their level of parental genetic relatedness21. There is a body of opinion which suggests that, through time, the practice of consanguineous marriage would have led to the effective elimination of detrimental genes from the South Indian gene pool.8 As with investigations into the association between consanguinity and fertility, many earlier studies were hindered by a lack of control for important sociodemographic variables, and in some cases the sample sizes were simply too small to allow adequate statistical analysis. Where appropriate clinical and laboratory investigations have been conducted, there has been no convincing evidence of a reduction in the prevalence of recessive lethals in the gene pool. The most recent representative estimate of consanguinity-associated mortality is based on a multi-national study of over 600,000 pregnancies and live births, in which 10 of the 38 populations studied were from India.23 The analysis showed that deaths from approximately the sixth month of pregnancy to a median age of 10 years were 4.4% higher in first cousin progeny than among the offspring of non-consanguineous unions. However, even this figure may be somewhat exaggerated as not all of the constituent surveys in the analysis had explicitly included control for potential confounding sociodemographic factors, e.g. maternal age, maternal education, birth order and birth interval. A comprehensive listing of genetic disorders that have been diagnosed in the progeny of consanguineous couples is presented at the website http//:www.consang.net. The diagnosis of birth defects may overlap with and reflect late fetal and neonatal survival rates. Also, the data that are available have been almost exclusively collected in the major cities and the majority of the population remains rural. Therefore reported prevalence rates may not necessarily be representative of the overall numbers of affected cases. Congenital disorders,24-26 including neural tube defects27,28 and congenital heart defects28-30 are more common in consanguineous progeny. Many different forms of autosomal recessive nonsyndromal hearing loss have been reported in consanguineous families world-wide although the data from India31 have been limited. By comparison, blindness caused by early onset retinal dystrophies,32,33 primary congenital glaucoma,34 anophthalmos and microphthalmos32,35 have been shown to be present at increased prevalence in consanguineous progeny. Similarly, both decreased IQ scores36,37 and increased levels of intellectual disability38,39 have been reported. Significantly, the prevalence of major infectious diseases including tuberculosis and leprosy are related to the HLA and other immune repertoires of different castes and sub-castes in South India, with caste endogamy and consanguinity probable contributory factors.40 A wide range of haematological disorders have been reported, in particular b-thalassaemia which occurs throughout the country, a-thalassaemia that mainly affects population in the north-east, and HbS that is largely restricted to tribal and scheduled caste populations.41 There also is an excess of cases of biochemical anomalies including amino acid disorders,42 glucose-6 phosphate deficiency,43 mucopoly-saccharidoses44 and cerebral lipidoses45 in children born to consanguineous parents. However, there is a paucity of national or even state level data for all of these disease states. A potentially more serious topic which has so far received little attention anywhere in the world is the possible effect of consanguinity on adult onset disease. Given the extremely high prevalence of premature coronary heart disease in South Asian males, an investigation of recessive genes as predisposing factors would appear to be warranted. In this respect, greater cooperation between medical researchers in India, and in countries where there are large Indian migrant communities, could usefully be employed to facilitate joint investigations.46 Discussion As indicated in Table 1, with the exception of Kerala there is little evidence of a recent overall decline in the prevalence of consanguineous marriage in South India. It is, however, probable that increased urbanization and the gradual shift to smaller family sizes will impose constraints on consanguineous marriage in future generations. The excess risk that an autosomal recessive disorder will be expressed in the progeny of a consanguineous union is inversely proportional to the frequency of the disease allele in the total gene pool.47 As previously discussed, the population of India is sub-divided into many thousands of endogamous communities that through time have evolved into distinctive breeding pools. The smaller the community the greater the probability that founder effect and genetic drift will exert a significant influence on the distribution patterns of specific mutations. Therefore, even in the absence of preferential consanguineous marriage, genetic isolation often results in an increased frequency of community-specific genetic disease.48 This fact is often overlooked, with the consequent general assumption that the presence of an autosomal recessive disease in a family or community at high frequency must be due to consanguinity. For example, in commenting on the elevated rates of recessive visual disorders reported in nine states of India,32 a call was made for the discouragement of consanguineous marriages as a means of reducing the prevalence of such disorders.49 Yet Table 2 shows that at state level there was no obvious association between the prevalence of inherited eye disorders32 and the levels of consanguineous marriage estimated in the National Family and Health Survey.12 This would suggest that in states such as Haryana recessive disorders may be present at high frequency because of founder effect and genetic drift, not consanguinity. However, to investigate whether this is indeed so it would be necessary to collect data at community level, as specific disease-associated mutations may be unique to individual Hindu castes and sub-castes, and to Muslim biraderis. The presence of multiple discrete sub-populations creates substantial practical difficulties in the preparation of disease registers and screening programmes for specific genetic disorders. On the positive side, once a specific mutation has been identified within a consanguineous pedigree, case ascertainment in other family members can be greatly simplified.50 This applies within communities that are effective genetic isolates, whether or not consanguinity is involved. Thus in a South Indian community it was possible to rapidly identify the causative mutation for the autosomal dominant disorder familial adenomatous polyposis coli, and to efficiently counsel and test all persons at risk.51 It should be stressed that genetic heterogeneity may persist even where a recessive disorder is known to be common within a particular inbred sub-population, with no guarantee that all affected members are homozygous for the same mutation. In addition, in many consanguineous isolates there also is the possibility that two or more mutant alleles are segregating within a family, which greatly complicates genetic counselling.47 The total burden of disease in a population can increase significantly as populations progress in economic terms, with the successful treatment of formerly lethal genetic disorders placing increasing demands on family resources. Thus, although consanguineous marriage may remain culturally desirable, a major shift in the balance between the social and economic benefits associated with intra-familial marriage and adverse health outcomes can be predicted. These changes are already underway in India and new diagnostic, counselling and treatment skills are urgently needed, alongside appropriate community education programmes.41,52 Since genetic disease already presents as a major national problem,52 it would be appropriate if programmes to determine the most prevalent genetic diseases in different parts of the country and in different sub-communities were initiated without delay. Acknowledgements An earlier version of this paper was presented at the Symposium on Community Genetics in Developing Countries, held in the Indian Institute of Science, Bangalore from January 16-18, 2002. The excellent technical assistance provided by Sheena Sullivan is acknowledged with gratitude. Generous financial support was received via an Australian Research Council Large grant and the Strategic Research Investment Programme of Edith Cowan University. References
Copyright 2002 - the Indian Society of Human Genetics The following images related to this document are available:Photo images[hg02010t1.jpg] [hg02010t2.jpg] |
| |||||||||

{kind=link}
{kind=link}