 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
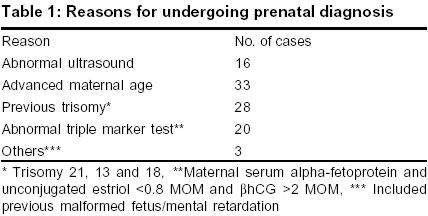
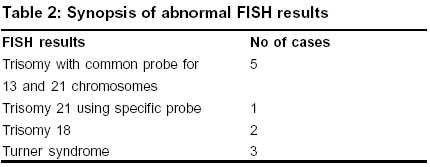
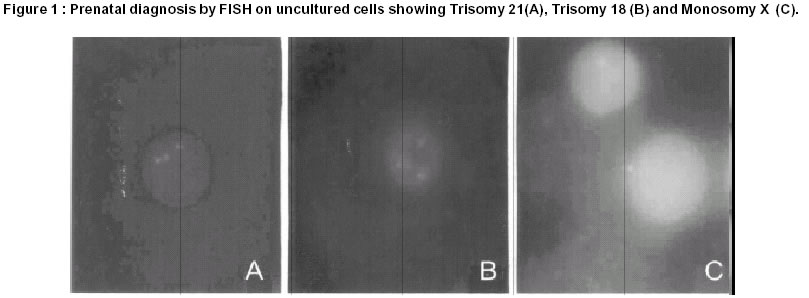
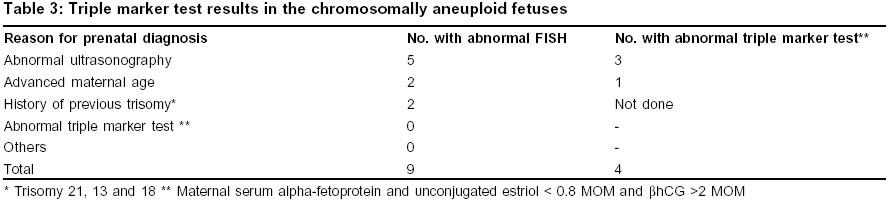
Indian Journal of Human Genetics, Vol. 8, No. 2, Jul-Dec, 2002 pp. 60-65 Clinical experience with the use of Fluorescence In Situ Hybridization on uncultured cells for prenatal diagnosis. Deepak N. Modi, Deepa Bhartiya Cell Biology Department, Research Society, Bai Jerbai Wadia Hospital for Children, AD. Marg. Parel Mumbai 400 012 India Code Number: hg02012 The aim of the study was to prospectively evaluate the usefulness and limitations of Fluorescence In Situ Hybridization (FISH) on uncultured cells for prenatal diagnosis of numeric aneuploidies of chromosomes 13, 18, 21, X and Y. Hundred prospectively selected pregnant women that were at high risk of giving birth to an abnormal child were offered prenatal diagnosis by FISH after appropriate counseling. Fetal tissue was obtained by chorionic villus sampling (n=26), amniocentesis (n=62) and or fetal blood sampling (n=12) and processed for FISH using commercial probes. Six cases were excluded initially owing to maternal blood contamination or inadequate sample. FISH results were available in 98% of cases, in 2% of cases there was FISH failure. Of the remaining 92 cases, chromosome aneuploidy was detected in eleven cases. FISH was found extremely valuable in cases presenting with fetal abnormalities detected on ultrasonography and also for rapid screening of aneuploidies in cases of abnormal triple marker test. But as the diagnosis is limited to only a small number of chromosomes, appropriate evaluation of the cases with counseling regarding the limitations of FISH is mandatory before offering this test for prenatal diagnosis. Key words: Prenatal diagnosis, fluorescence in situ hybridization, FISH, chromosome aneuploidies Introduction Every couple desires a normal baby, bringing up genetically abnormal child poise a great deal of socio-economic burden on the parents and the family. The field of prenatal diagnosis (PND) has undergone rapid advances because of which it is now possible to consider the fetus as a patient who can be studied in utero for various genetic defects. Amongst the various reasons for which an expectant mother undergoes prenatal diagnosis for chromosomal defects are advanced maternal age (>35 years), previous child with chromosomal defects, balanced chromosomal aberrations in either of the parents, structural abnormalities detected in the fetus on ultrasonographic viewing and or abnormal triple marker test report (low maternal serum alphafetoprotein, and unconjugated estraiol and increased free beta hCG).1,2 The various fetal samples available for PND for chromosomal disorders are chorionic villi, amniotic fluid cells and fetal blood. Cytogenetic analysis by conventional microscopic analysis of banded metaphase chromosomes involves setting up of cultures of chorionic villi sample (CVS) or amniotic fluid cells or lymphocytes from fetal blood sample (FBS). This method is accurate and permits detection of numerical and structural aberrations of chromosomes. However, cytogenetic analysis requires a great deal of technical expertise, tissue culture facilities and a long waiting period for results. It takes a minimum of 2 weeks to obtain the cytogenetic report from a CVS or amniotic fluid cell cultures.3 This long waiting period is singularly a major shortcoming, as in clinical situations there exist many cases where a rapid report is desired to take a decision and action. It has been observed that in cases of prenatal diagnosis when the legal limit for termination of pregnancy is near, rapid results are highly desirable by the clinicians and the parents.4 Also, in cases of abnormal triple test reports or abnormal ultrasound the parents4,5 undergo extreme anxiety and rapid diagnostic reports are desirable.1,4 Although direct chromosome preparations from CVS is a rapid method for cytogenetic analysis, the number and quality of chromosomes obtained are often poor. Furthermore, most cases of abnormal ultrasound and abnormal triple test reports present in the second trimester when CVS is not desirable. Cytogenetic analysis from FBS is also relatively rapid and good metaphases are obtained but the process of FBS is safe only in the late second trimester (~18 weeks). However, if medical termination of pregnancy is needed, it is unsafe for the mother and is not accepted in many communities. Hence a rapid and accurate method for prenatal chromosome analysis is a long sought goal of medical cytogenetics. One of the promising methods to detect chromosome aneuploidies that have become available due to advances in the field of Molecular Biology is Fluorescence In Situ Hybridization (FISH). The FISH technique involves use of chromosome specific labeled DNA probes that identifies chromosomes and chromosomal domains in interphase and metaphase spreads. Also known as `Interphase Cytogenetics' FISH can diagnose numerical anomalies of chromosomes rapidly in a highly sensitive and specific manner as it does not involve setting up of cultures. Therefore results are made available quickly and failure rates are also very low. Furthermore, large number of cells can be analyzed, as signals are detected in interphase cells.6 These features of FISH make it an attractive technique for prenatal diagnosis of chromosome abnormalities. Since aneuploidies of 13, 18, 21, X and Y chromosomes account for 90-95% of all live born chromosomal abnormalities7 various groups have used FISH to provide prenatal diagnosis using probes for these five chromosomes. Extensive studies have been carried out for prenatal diagnosis using FISH.4,7,8-12 All these studies have compare the efficiency of FISH to conventional cytogenetics and the results suggest that FISH is an efficient and rapid tool for prenatal diagnosis of chromosomal disorders and is a useful adjunct to karyotyping. In fact, the American Society of Medical Genetics13 recommends the use of FISH for prenatal diagnosis in addition to karyotyping. Retrospective analyses have suggested that FISH alone is sufficient for prenatal diagnosis in certain high-risk situations such as fetal abnormalities detected on ultrasonography.4 Despite these recommendations and the high efficiency of FISH, to the best of our knowledge very few prospective studies have been carried out to evaluate the usefulness of FISH alone for prenatal diagnosis in high-risk situations. In the present study we describe our experience with the use of interphase FISH alone for prenatal diagnosis of chromosome aneuploidies. The purpose of the study was to prospectively evaluate the usefulness and limitations of interphase FISH for chromosomes 13, 18, 21, X and Y for prenatal diagnosis Material and Methods The present study was conducted over a period of three years (August 1997 to July 2000). A total of one hundred high risk women were offered prenatal diagnosis using FISH test after appropriate counseling of the couples especially regarding the limitations of the test. Written informed consent was obtained from all cases before testing. The reasons for which the patients opted for PND are listed in Table 1. The sample collection was done under ultrasound guidance using a 21 gauge sterile disposable needle with stylett without anesthesia on OPD basis. A total of 26 CVS, 62 amniocentesis and 12 cord blood sampling were carried out to obtain fetal cells. There was no fetal loss noted due to these procedures. All the women were followed up until delivery and the newborn examined by the neonatologist and or a clinical geneticist. Sample processing Chorionic villi were dissected carefully to remove maternal decidua, presence of which would lead to misdiagnosis.14 Amniocytes were isolated by centrifugation and washed twice in saline. Lymphocytes from cord blood were separated on Ficoll Hypaque (Sigma USA). After washing the chorionic villi threads, amniocytes and lymphocytes were processed according to standard cytogenetic protocols. Briefly, the cells were given hypotonic treatment with 0.075 M KCl for 30 minutes at 370C followed by fixation in Carnoys fixative (3:1 methanol : acetic acid) for at least 4 hours. The cells from villi were dissociated using 60% acetic acid prior to fixation. The fixed cells were spread on aminosailine coated slides and air-dried. To increase the permeability of the cells and improve the signal to noise ratio, the chorionic villi cells and aminocytes were treated with Triton X-100 (0.3%) for 15 minutes and proteinase K (2.5 mg/ml, Gibco BRL, USA). This was followed by a second fixation in 4% paraformaldehyde (Sigma, USA) containing 5mM magnesium chloride. Lymphocytes from FBS were treated only with proteinase K for 10 minutes prior to fixation. Amniotic fluid cells that were visibly contaminated with blood or RBCs detected after centrifugation of the amniotic fluid were excluded for FISH as it could have maternal blood cells that could lead to misdiagnosis.9 Chromosomes probes DNA probes specific for chromosomes 13, 18, 21, X & Y were initially purchased from Amersham (UK) and subsequently from Vysis (USA). Initially a common probe for chromosomes 13 & 21 was used (Amersham UK) but later we used specific probes for chromosomes 13 & 21 (Vysis USA). FISH protocol FISH was carried out using the procedure described previously.15 Briefly, the protease digested cells were incubated in 2XSSC for 30 minutes at 370C followed by dehydration in grades of ethanol and air-drying. The target DNA in the cells was denatured in 70% formamide at 750C for 8 minutes. The cells were dehydrated again and air-dried. Simultaneously, the probe was denatured in the hybridization cocktail (65% formamide, 2XSSC, dextran sulphate and sheared salmon sperm DNA) at 750C for 5 minutes and snap frozen. 8 microliters of the denatured probe was applied on to the slides and hybridization was carried out at 420C for at least 4 hours. The slides were then stringently washed and mounted in antifade medium (2.3% DABCO containing DAPI as counterstain). The above procedure was modified by performing codenaturation of the target cells and the probe. In this case the undentured probe was applied on to the dehydrated cells and the slide was left for denaturation at 750C for 5 minutes and hybridized, washed and mounted as above. The slides were viewed under a fluorescent microscope (Olympus BX 60) at 100X magnification using appropriate filters. The signals were directly photographed using a 400 ASA Kodak Gold color film. Image analysis system was not used in this study. FISH analysis A minimum of 50 amniocytes or 200 CVS or lymphocytes cells were scored according to standard criteria.9,10,15 We considered the FISH results informative if and only if 80% of amniocytes or 95% of lymphocytes showed a consistent diploid pattern. The fetus was considered as affected if at least 70% of amniocytes or 80% of CVS or lymphocytes cells were aneuploid. Any sample failing to reach this expected cut off was deemed uninformative. These criteria have been used previously by us and other groups.8-12,15 For the purpose of standardizations, FISH was performed on lymphocytes of 10 normal males 10 normal females, 4 amniotic fluid samples and 5 CVS samples. The amniotic fluid and CVS samples were obtained from a aliquot samples collected at our institute for PND for other reasons. The rates of false positive and negative values obtained has been reported elsewhere.15 Results FISH results were made available within 48 72 hours of sample collection. According to the criteria described in the material and method section, five cases were excluded from the study, as there was visible blood contamination in the amniotic fluid cells. One case of CVS was not analyzable due to inadequate sample. In two of the remaining 94 cases, FISH results were uninformative as the pattern of signal distribution failed to reach the expected cutoff. Notably, in both the cases amniocytes were used as source of fetal cells and the uninformative results were in case of probe 13/21 (Amersham probes) in one patient and chromosome 13 alone (Vysis probe) in case of other. The results using other probes were normal in both the cases. The overall rate of unavailable diagnosis was 8% and the FISH failure rate was 2%. The probe specific FISH failure rate was nil in cases of probes 18, X and Y whereas it was 2% in case of 13 and 21 in combination. Four of the eight cases where diagnosis was unavailable chose to have a repeat sampling done and all the cases were normal. Eighty-five cases had a normal FISH report and a normal pregnancy outcome. Eleven cases revealed an abnormal FISH result (Table 2). Fig 1 represents FISH results on amniocytes and cord blood lymphocytes in 3 cases diagnosed to have trisomy 18, trisomy 21 and monosomy X respectively. Five cases had trisomy 13 or 21 (using the 13/21 common probe), one case had trisomy 21 by the specific probe (Fig 1A), two cases had trisomy 18 (Fig 1 B) and 3 cases had XO i.e. Turner syndrome genotype (Fig 1C). Of the five cases that revealed presence of trisomy 13/21 (using a common probe for chromosomes 13 & 21) two were found to be false positives as in both these cases simultaneous karyotyping (done elsewhere) gave a normal report and babies were born normal. Remaining nine cases were confirmed to be affected by FISH and karyotyping of fetal tissue after termination. Five out of the eleven cases diagnosed as affected had malformations on ultrasound. The remaining eleven cases with malformations on ultrasound (Table 1) had a normal FISH report and gave birth to chromosomally normal babies. The malformations detected in these cases were minor or nonspecifically associated with the disorders of chromosomes 13, 18, 21 X and Y. For example, in one case ultrasound report indicated the presence of diaphragmatic hernia (condition generally found associated with trisomy 21 or 18) was chosen for FISH analysis for obstetric reasons at 32 weeks of gestation. FISH on amniotic fluid cells from this case indicated absence of trisomy 13, 18 and 21 and the baby born by a cesarean section was promptly provided surgical care. Among the other categories we did not detect abnormalities of chromosomes 13, 18, 21, X and Y in any of the patient with abnormal triple marker test. Two cases with advanced maternal age had chromosome abnormalities and two cases with previous history of an abnormal child had aneuploid fetuses (Table 3). To test if the fetuses diagnosed to be affected had an additional risk apart from that for which PND was opted (Table 1), we performed correlation studies with abnormal triple marker test. Of the 9 cases in whom the chromosome abnormality was detected, triple test results were available5 in seven cases. Four of the seven cases had the double risk (Table 3). Discussion In the present study we have used FISH successfully for giving prenatal diagnosis of aneuploidies related to chromosomes 13,18,21, X and Y using uncultured cells. Several workers have reported usefulness of this procedure in the field of prenatal diagnosis.4,6,8,9,11,12,16 However, it is well accepted that FISH cannot replace cytogenetics that allows the analysis of all the chromosomes. D'Alton and co-workers4 have proposed that due to the high accuracy of FISH on uncultured cells in high risk cases such as those near the legal time limit for medical termination of pregnancy, an informative FISH could be used together with an abnormal ultrasound for management decisions without waiting another 7-14 days for karyotype report. Although extensive debate is going on this issue17 our results support this notion as FISH diagnosed all the fetuses with malformations having chromosomal abnormalities. The remaining normal cases had either single defects like increased nuchal fold thickness or diagrammatic hernia that are associated, although less frequently with chromosome abnormalities. Our results also suggest that FISH can also be diagnostically useful in cases of double risk situations like advanced maternal age with abnormal triple marker test reports. In these situations a rapid evaluation of chromosome aneuploidies by FISH is desirable as the patients suffer from extreme anxiety.4,5 A proper and well-planned combination of the triple test with FISH in screen positive cases could bring down the incidence of aneuploid births.5 In any case it is safe to be cautions while offering this test to a couple. In our experience prior extensive counseling is very essential that point out both, limitations (only restricted diagnosis of chromosomes 13,18,21 X and Y) and advantages (rapid report of FISH) to the patient before offering the test in place of karyotyping. Since FISH can also miss out other abnormalities that are detected by routine karyotyping17 it is not possible that FISH can completely replace karyotyping. But in some deserving cases where the suspected abnormality needs to be confirmed, FISH can be of great assistance. Thus we propose that the obstetrician, the clinical geneticist and the cytogeneticst to coordinately evaluate the case and a final decision for the technique for PND is taken after counseling the patient. A similar strategy has also been proposed by Hogge et al.16 Indeed following this strategy we were able to offer quick diagnosis to a deserving group of patients. In our experience a proper counseling especially regarding the limitations needs to be pointed out as, from our cohort two couples opted out of the study after noting the limitations. A second limitation of FISH in use for PND is the uninformative result. Although, in the initial studies, the uninformative rates were high8,9 but with the commercialization of the FISH probes the rate of uninformative FISH us reduced considerably.4,11,12 The overall uninformative FISH rate in the present study was 8% with FISH failure rate of 2%. This overall rate of undiagnosed cases (8%) is somewhat higher, but the uninformative rate owing to sampling procedure can be reduced by carefully performing amniocentesis to avoid blood contamination. After our initial experience we routinely discarded first 5 ml of amniotic fluid after needle injection, the subsequent fluid obtained in most cases is clear and useful for FISH. In the initial phase of the study (n=20 cases) where a common alpha satellite probe for chromosomes 13 and 21 were used we came across two false positive diagnoses. This indeed gave a setback to our study. But rather than a technical problem, it was realized that this probe along with chromosome 13 and 21 also cross hybridize with chromosome 22 in some cases giving false positive results.18 Hence we subsequently (n=80 cases) used the chromosome specific probes and no false positive or negative cases were encountered. This experience highlights the need for carefully selection and probe sets and stringent reporting criteria to avoid false results In conclusion the present study shows that FISH test alone can be used for giving prenatal diagnosis in high-risk situations. Well-designed multi centric prospective studies are further warranted and regulatory guidelines needs to be established by the competent government bodies for the use of this technique for prenatal diagnosis. Integration of FISH in to routine antenatal practice in future will be able to offer prenatal diagnosis to more number of cases to have normal healthy babies. It is therefore imperative that more laboratories should develop expertise in this relatively simple, reliable and quick test for identification of chromosome anomalies. Acknowledgements We are grateful to Department of Biotechnology, Govt. of India and Smt Trikadevi Kedarnath Kapur Foundation, Mumbai, India for financial assistance. We express our gratitude to Dr PG Natrajan (Nanavati Hospital Mumbai)and the clinicians of Navrosji Wadia Maternity Hospital (Mumbai) for referring cases to us. We are thankful to Dr. S.G. Gangal (Former Director BJWHC) for her help and expert guidence. References
Copyright 2002 - the Indian Society of Human Genetics The following images related to this document are available:Photo images[hg02012t1.jpg] [hg02012f1.jpg] [hg02012t3.jpg] [hg02012t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}