 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Human Genetics, Vol. 9, No. 1, Jan-Jun, 2003, pp. 5-9 Review Article Alternate strategies for carrier detection and antenatal diagnosis in haemophilias in developing countries Shrimati Shetty, Kanjaksha Ghosh, Dipika Mohanty Institute of Immunohaematology (ICMR), K.E.M. Hospital, Parel,
Mumbai-400012
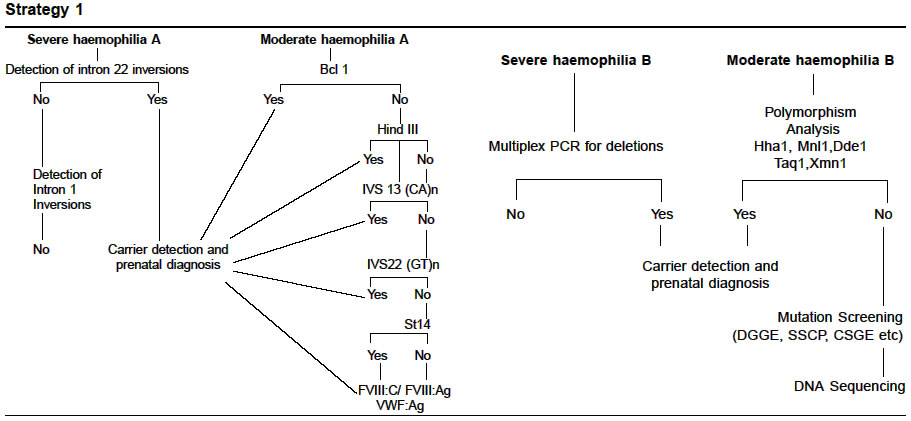
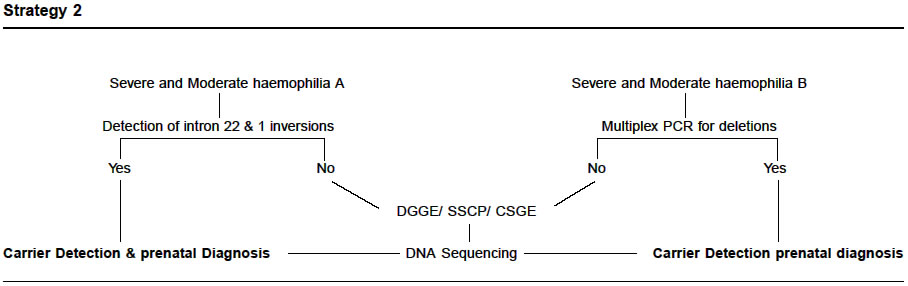
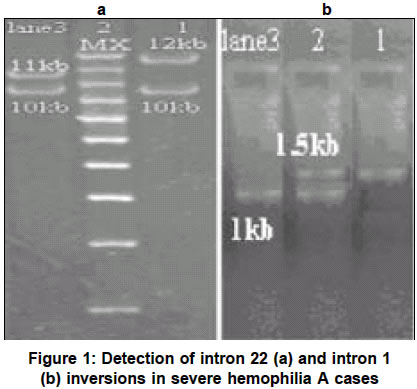
Code Number: hg03002 Carrier detection and prenatal diagnosis constitute an important component of haemophilia management . Recent advances in molecular biology allows us to use the tools of molecular biology to give such a diagnosis early in the pregnancy with a much higher confidence. Because of lyonisation, diagnosis of a carrier by factor assay is imperfect and hence lacks sensitivity. Molecular diagnosis in such cases is robust.There are several techniques by which this diagnosis can be made.Though the preferred method is to do direct mutation studies, yet the complexities of factor VIII and factor IX genes may not make this approach easy or cost effective. Hence depending on the capability of the laboratory, education status of the family, availability of data through several generations and economic situation of the country, a combination of these techniques need to be adopted for optimum results. These techniques are broadly classified as indirect techniques through linkage analysis or direct detection of affected genes by a combination of screening and sequencing techniques. Occasionally in our country even all the gene based techniques may prove inadequate and we may have to give prenatal diagnosis by antigen and clotting activity assay of the defective factor by cordocentesis between 17-20 weeks of gestation. For any prenatal diagnosis of haemophilia, prior detection of fetal sex either by USG or by molecular technique is necessary to decide whether any further work up is necessary or not? The present article describes various algorithms of carrier detection prenatal diagnosis of haemophilia that was found suitable in our country. Key Words: Hemophilia, carrier detection, prenatal diagnosis, developing countries. INTRODUCTION Hemophilias are X-linked, recessively inherited bleeding disorders caused by heterogeneous mutations of factor VIII / IX genes,1,2 identification of carriers, antenatal diagnosis and genetic counselling are important aspects of hemophilia care and the effective control of the disease. Genetic diagnosis is usually achieved by linkage analysis using restriction fragment length polymorphisms (RFLP) or short tandem repeats (STRs) to track the defective allele in the affected families.3 Though linkage analysis is technically straight forward, yet the method has certain limitations in its application in families lacking a prior history of hemophilia and / or informative polymorphic makers. In cases of severe hemophilia A, direct detection of intron 22 inversions of the factor VIII gene explains almost half of severe patients4,5 and intron 1 inversions are detected in about 1-5% of severe hemophilia A cases.6,7 A spectrum of other pathological defects including point mutations, deletions, insertions have been reported in both hemophilia A and B which is characterized by an extensive heterogeneity and relatively high rate of de novo mutations. Due to the severity of the disease which can often be complicated by development of inhibitors8,9 transfusion transmission disease,10,11 genetic counselling and diagnosis are often requested by affected families. The cloning and complete characterization of factor VIII / IX genes now permits the diagnosis of the affected fetus and carrier status by DNA analysis. Two broad approaches are used to offer genetic diagnosis in hemophilia. a. Indirect method This is based on the analysis of DNA polymorphisms associated with factor VIII / IX genes. Commonly used makers are within the introns or close to the genes. Most under study. A number of factors have complicated this kind of study,most important of these is the fact that both factor VIII / IX genes are large i. e. 186 Kb and 33 Kb respectively and complexity of its genomic organization. A further complicating factor is marked mutations heterogeneity that has been documented over the years. Nevertheless detection of gross gene rearrangement in the factor VIII gene i. e. intron 22 and intron 1 inversions has made the director mutation detection possible in about half of the cases of severe haemophilia. Although prevalence of intron 1 inversions has been found to the relatively low, when individual family is non informative for all the markers and intron 22 inversions detection of this event might prove to be highly useful for the family. In the intron 22 inversion negative severe cases and in moderate to mild disease cases, the disease is caused by large number of infrequent mutations i.e. point mutations, deletions and insertions. These mutations can be directly detected by sophisticated and expensive DNA sequencing strategies. Various mutation screening protocols are available like denaturing gradient gel electrophoresis(DGGE),16 single strand conformation polymorphism (SSCP),17 conformation sensitive gel electrophoresis (CSGE),18 heteroduplex analysis which may be performed prior to DNA sequencing analysis. This would in the first step show an aberrant migration profile in a particular segment which then would be directly sequenced to understand the nature of the mutation. Dinucleotide Repeat Analysis There are a range of different procedures available for the analysis of dinucleotide repeats depening on the availability of of sources available. Simplest method is to electrophorese the PCR products on a polyacrylamide gel and then stain with ethidium bromide or silver to visualize the products. Radiolabelling one amplification primer with P32 prior to PCR is the widely used technique.12 The PCR products are electrophoresed on a denaturing sequencing gel and visualized by autoradiography. However some of the laboratories have logistical problems with the use of radioactivity in the laboratory and would prefer to use nonradioactive detection methods. A protocol for automated genotyping has also been reported.19 Inversions in the factor VIII gene Intron 22 inversions can either be detected by Southern blotting 4 or by long template PCR technique20 whereas intron 1 inversions can be detected by a simplified PCR protocol6 (Figures 1a & b ). RFLP analysis The polymorphic marker analysis is done for both factor VIII and IX genes by PCR with or without restriction enzyme digestion.3 Multiplex PCR for the detection of large deletions A PCR protocol for the detection of large deletions in the factor IX gene has been described.21,22 Using 9 pairs of primers which encompasses the entire factor IX gene a multiplex PCR is performed to detect the large deletions. Measurement of factor VIII/ IX coagulant activity and antigen levels Prenatal diagnosis using factor VIII / IX activity and/or antigen assay on umbilical cord blood obtained by cordocentesis at 18-20 weeks of gestation23 has been largely given up due to the superior results obtained by molecular biological techniques. However this technique has been found to be useful in many laboratories including that of ours when i. carrier mother did not carry intron 22 inversions of factor VIII gene in caases of severe haemophilia A ii. sporadic families where the mothers carrier status is
uncertain
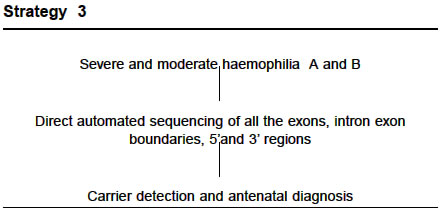
The ratio method of factor VIII:C / VWF : Ag has been found to be accurate in about 90%of our carrier population in haemophilia A families.24 These are extremely useful as a complementary data in cases where the diagnosis is offered using extragenic markers. In some cases, the factor VIII : C activity alone (<30% of the normal) provides a fairly good clue whether the female under investigation is a carrier or not. CONCLUSION Genetic counselling of patients with severe haemophilia and their relatives is an important part of the clinical management of this disease. In this regard, the molecular biological protocols have significantly improved the accuracy of carrier detection and prenatal diagnosis of the disease. Analysis of intron 22 inversions which explains approximately half of the severe cases of haemophilia has become a routine test in majority of the laboratories, as there is a PCR protocol for detecting these inversions. Intron 1 inversions though less prevalent, because of the simplicity of the test should be looked into because if a family is informative for these inversions then a direct detection is possible here in either the fetus or a female who needs her carrier status. Polymorphism analysis when involves intragenic markers is a highly useful, cost effective and accurate test but caution should be exercised when extragenic markers are being used. Direct detection of causative mutations enables female carrier status to be determined in all the females irrespective of prior disease history in the family. Various point mutation screening techniques are now available which are quite simple wherein the amplified DNA fragments show altered gel migration under specific conditions, if mutations are present. These may then be sequenced to characterize the change and identify whether it is polymorphic or likely to be the causative mutation. Mutations are then sought in at risk female family members to determine the carrier status. Thus several molecular strategies have been described and reported for the genetic diagnosis of haemophilia. Direct mutation screening or automated sequencing which is now become a routine practise in the western countries may look appealing as it directly detects the molecular pathology and does not require other family members, but it may not be practically applicable in the developing countries. Each laboratory in the developing country should develop a strategy depending on the availability of resources, technical expertise and sensitivity of the various tests. Prenatal diagnosis by measuring factor VIII:C / IX:C and antigen levels may be an outdated technique in other countries but in the developing countries it still has retained its significance owing to various factors like presentation at advanced pregnancy, unavailability of a detailed family history, absence of the index cases and absence of informativeness with the polymorphic markers. REFERENCES
Copyright 2003 - the Indian Society of Human Genetics The following images related to this document are available:Photo images[hg03002s1.jpg] [hg03002f1.jpg] [hg03002s2.jpg] [hg03002s3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}