 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Human Genetics, Vol. 9, No. 2, July-Dec, 2003, pp. 65-68 Plasma Lipoprotein (a) levels in patients with untreated essential hypertension B. A. Bhavani, T. Padma, B. K. S. Sastry,* N. Krishna Reddy* Department of Genetics, Osmania University, Hyderabad, India;
and *Department of Cardiology, CARE Hospital, Nampally, Hyderabad, India.
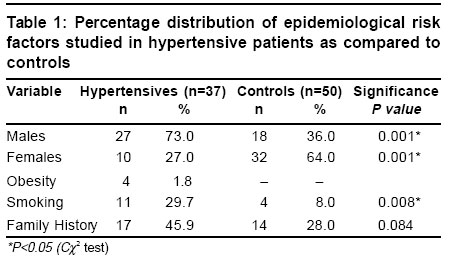
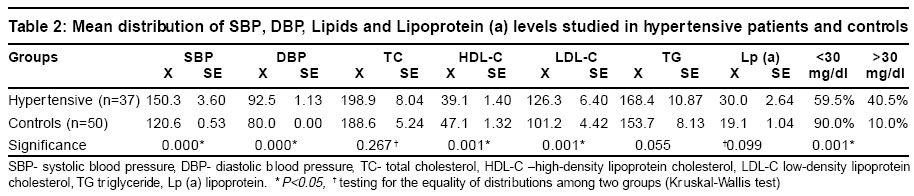
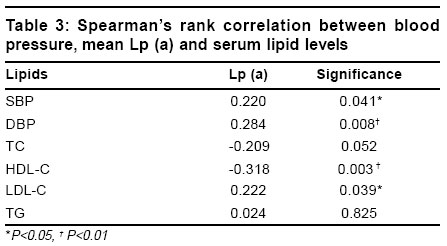
Code Number: hg03013 Lipoprotein (a) [Lp (a)] is considered as a risk factor for vascular diseases, especially those associated with renal failure. Adequate studies have not been conducted on the lipoprotein (a) in essential hypertensive patients. There is a controversy on the mechanisms by which Lp (a) is associated with essential hypertension. It is unclear whether Lp (a) contributes to atherogenesis or to thrombogenesis or both. Recent studies suggest that Lp (a) can act as a marker for determining vascular or tissue injury. Reports on Indian population indicate elevated levels of Lp (a), together with other serum lipoproteins emphasizing an important role in Coronary Heart Disease (CHD) and peripheral atherosclerosis. In the present study we aimed to evaluate the relation between plasma levels of Lp (a) and the parameters of the lipid profile in a group of essential hypertensive patients, who are not receiving pharmacological treatment and with no clinical signs of associated pathologies or organ damage. A total of 37 essential hypertensive patients (27 men and 10 women) were compared with 50 controls (32 men and 18 women). It was observed that the hypertensive patients had higher plasma concentrations of Lp (a), Total Cholesterol (TC), Low-Density Lipoprotein-Cholesterol (LDL-C), and Triglycerides (TG) as compared to controls (P< 0.01). Hypertensive patients were also observed to have significantly low levels of High-Density Lipoprotein Cholesterol levels (HDL-C) as compared to controls (P<0.01). Only 14 hypertension patients and 4 controls had plasma concentrations of Lp (a) of over 30 mg/dl. Lp (a) values correlated significantly (P<0.05) with systolic blood pressure (SBP), diastolic blood pressure (DBP) and the main parameters of the lipid profile. We conclude that elevated plasma Lp (a) levels were associated with hypertension and show significant correlation with lipid levels. However higher plasma concentrations of Lp (a), albeit with in the normal range, could be an independent risk factor for atherosclerosis, and could contribute towards increasing the risk for cardiovascular disease in persons with essential hypertension. Key Words: Essential hypertension, Lipids, Lipoprotein (a). Introduction Cardio vascular diseases (CVD) have emerged as a global health problem. Essential hypertension (EH), one of the major risk factor for CVD is posing a health challenge by topping the list of killer diseases due to the associated target organ damage. Several prospective studies have identified the major risk factors for hypertension like obesity, smoking and alcohol consumption, dyslipidemia apart form dietary patterns. There are very few studies that have shown the importance of other genetically determined as well as acquired risk factors in the pathogenesis of essential hypertension and its susceptibility to CVD. Lipoprotein (a) is a complex lipoprotein macromolecule that contains apolipoprotein (a), which shares homology with plasminogen.1,2 It acts as a competitive inhibitor of tissue type plasminogen activator and there by helps in modulating the fibrinolytic system consistent with an atherogenic role.3,4 Lp (a) levels are known to exhibit significant inter individual variation and are strictly under genetic control. Elevated serum Lp (a) levels are associated with an increased risk of cardiovascular disease and renal failure in hypertensive patients, but only if LDL levels are also high.5,6 As Lp (a) levels are genetically determined, screening for Lp (a) levels in asympotomatic individuals has been suggested7 to identify the subjects at risk. There are very limited case-control studies determining association between Lp (a) excess and essential hypertension. In the present study we aimed to investigate the possible relationship of plasma Lp (a) levels and lipids and also to evaluate the role of Lp (a) in assessing risk for hypertension and organ damage. We specifically chose to study hypertensives, who were not receiving any treatment since antihypertensive drugs can influence the lipid levels and enmask the presence of correlation with Lp (a). Material and Methods A total of 37 essential hypertensive patients (27 men and 10 women), with in the age group of 35-60 years, without any associated conditions were studied by visiting the CARE hospital-a Cardiac Center, Hyderabad. Hypertension was diagnosed according to WHO guidelines.8 50 randomly selected healthy controls (32 men and 18 women) with in the same age group (35-60 years) were also studied for Lp (a) levels. Both patients and controls were interviewed about the history of diabetes (DM) or Coronary Artery Disease (CAD), current use of antihypertensive medications, smoking, history of alcohol consumption, etc. Essential hypertension was confirmed on the basis of routine laboratory investigations like complete blood picture, urine examination, ECG, X-ray, 2D Echo etc and cases with secondary hypertension, organ damage and those under medication were excluded from the study. Venous blood samples were obtained from all the patients, with their consent, after 12 hours of fasting. Total cholesterol (TC), High Density Lipoprotein- Cholesterol (HDL-C) and Triglycerides (TG) in plasma were measured by enzymatic methods using commercially available kits (Wipro BIOMED, Bangalore; HUMAN, Germany; Merc limited, Mumbai respectively). Low-Density Lipoprotein- Cholesterol (LDL-C) was calculated by Friedewald's9 formula. Lp (a) levels were estimated by invitro turbidometric immunoassay using a kit (WAKO PURE chemical industries Ltd). Body mass index (BMI) was calculated as weight in kilograms divided by the square of the height in meters and a value of >30 is considered as measure of obesity. All epidemiological and biochemical data were recorded prospectively. We compared Lp (a) levels of patients with those of controls. Previous reports have suggested that >30 mg/dl of Lp (a)10,11 is the threshold value linked to its pathological effects. Based on this value, we defined subjects with >30 mg/dl as those with high levels of Lp (a) and examined its frequency in hypertensive patients and controls. We also studied the association of high Lp (a) with epidemiological variables and lipid profile. Continuous variables were reported as mean + standard error. The difference in mean values between groups was tested by 2-tailed t-test for parametric data. The difference in categorical variables was compared with the use of the chi-square test. The statistical analysis was done using the SPSS package (Ver 10.0). As distribution of mean HDL-C and Lp (a) levels were found to be highly skewed non parametric tests like kruskal-Wallis test12 was applied to test for the significance of difference between the patient and control groups. Correlations between SBP, DBP, the various lipid levels like TC, HDL-C, LDL-C and TG and Lp (a) were calculated by using Spearman's rank correlation coefficients. A value of (P<0.05) was considered significant for all the tests of significance performed. Results Base line characteristics of hypertensive patients and healthy controls as observed in the present study are described in table 1. Hypertensive patients were observed to show significant differences when compared to control groups with respect to sex, obesity and smoking (P<0.01). The two groups were similar with respect to presence of family history. Table 2 shows the mean distribution of SBP, DBP, lipids and Lp (a) levels in hypertensive patients and control group. It was observed that mean levels of SBP, DBP, TC, LDL-C and TG were elevated in hypertensives when compared to controls, but HDL-C levels were significantly reduced. (P<0.01). Though mean levels of Lp (a) were elevated in patients, did not reveal any significant differences from controls. Lp (a) levels >30 mg/dl is generally considered as the threshold value of high risk for its pathological effect. In the present study taking >30 mg/dl as the cut off value, majority of the patients (40.5%) had levels >30 mg/dl (P<0.01) when compared to controls (10%, Table 2). The correlations between Lp (a) concentration, SBP, DBP and other lipids as observed in hypertensives are summarized in table 3. Lp (a) values correlated significantly with SBP, DBP, HDL-C and LDL-C levels in the present study, which is in consistence with other investigations.13,14 Discussion In the present study, it was found that the hypertensive patients had higher plasma concentrations of Lp (a) than in the controls. In a similar study, Catalano et al15 reported significantly elevated levels of plasma Lp (a) in 123 Caucasian essential arterial hypertensive patients (47 men and 76 women). Studies in Indian population have shown that Lp (a) levels are significantly higher among pulmonary arterial hypertension16 (mean 31.6 mg/dl). Recent report from Fytili et al6 suggested that arterial hypertension is associated with elevated Lp (a) levels in patients of end stage renal disease. In their study it was observed that Lp (a) levels were significantly higher in the hypertensive patients, but that difference was not significant among non-renal failure patients. This observation is in compliance with that of present study. Studies in Indian population also reveal that Lp (a) levels are significantly higher among coronary artery disease (CAD) patients as compared to controls.17-19 Mohan et al20 showed that Lp (a) was an independent risk factor for CAD in diabetic patients. In previously reported studies on Indian subjects21-23 the mean values have ranged from 15.0 mg/dl to 34.0 mg/dl in healthy controls and 20.90 mg/dl to 41.0 mg/dl subjects involving seven ethnic groups. Lp (a) levels were almost twice as high in Indians as compared to Caucasians, Malays, and Chinese residents of Singapore.24 In the CADI study on the Immigrant. Indian population Lp (a) levels > 30 mg/dl were found in a higher proportion of Asian Indians as compared to whites (25% Vs 17%)7,25 prompting the conclusion that Indians are at a greater risk for CAD. It has been observed by several investigators that Lp (a) levels are highly variable showing bimodal distribution among subjects.26 In the present study, majority of hypertensive patients had levels >30 mg/dl which in general, is taken as high-risk level for atherogenesis. It needs to be confirmed using larger sample whether this population has more number of individuals with Lp (a) >30mg/dl. Mohan et al20 in their study found 57% of NIDDM patients with CAD exhibiting Lp (a) level > 30 mg/dl as compared to 36% of NIDDM patients without CAD and 30% of control patients suggesting elevated Lp (a) levels could be a potent risk factor for atherogenesis.. In a similar study by Catalano et al15 it was found that in Caucasians only 13% of hypertensive patients had Lp (a) > 30 mg/dl when compared to 8% in controls. The frequencies observed in the present study are quite high (40.5% in patients and 10% in controls) when compared to the Caucasian population. The pathogenicity and atherogenic role of Lp (a) is greatly influenced by the concentration of other serum lipids and lipoproteins.14,19 Several investigators reported correlation between Lp(a) and other lipid variables. In the present study a significant correlation was observed between HDL and LDL cholesterol levels and Lp (a). This observation was compatible with study from Beena et al19 but not consistent with the study from Caucasians in which no correlation was observed.15 We could confirm that hypertension and dyslipidaemia, which are two of the main risk factors for vascular diseases on atherosclerotic basis, are often associated. However, higher plasma concentrations of Lp (a), though with in the normal range, could be an independent risk factor for atherosclerosis, and could contribute towards increasing the incidence of Cardio-Vascular Disease in persons with essential hypertension. In conclusion the increasing mortality due to hypertensive end stage organ damage, emerging as an epidemic among the population of India is greatly debatable. We need to identify susceptible individuals and adopt preventive measures. New therapeutic methods may be identified to reduce Lp (a) levels, which may prove to be useful in patients with essential hypertension. References
Copyright 2003 - the Indian Society of Human Genetics The following images related to this document are available:Photo images[hg03013t3.jpg] [hg03013t1.jpg] [hg03013t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}