 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
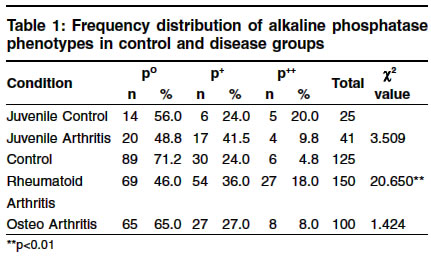
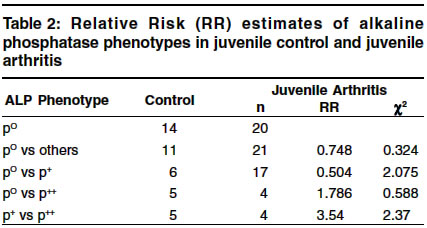
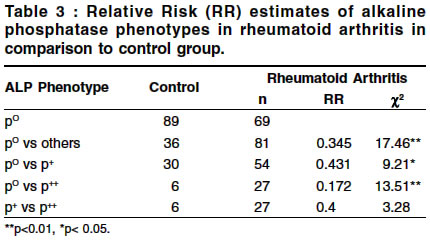
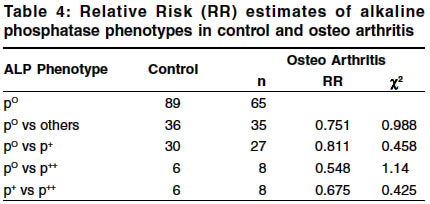
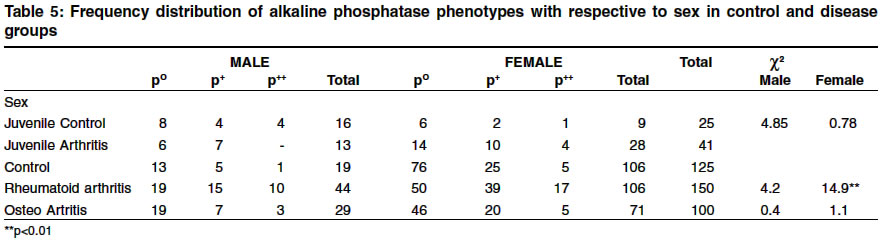
Indian Journal of Human Genetics, Vol. 10, No. 1, Jan-June, 2004, pp. 5-8 Original Article Association of alkaline phosphatase phenotypes with arthritides Padmini A, Ushasree B, Babu Ravi , Nallari Pratibha Department of Genetics, College of Science, Osmania University, Jamai Osmania Post office, Hyderabad - 500 007 Code Number: hg04002 ABSTRACT Arthritides, a symmetrical polyarticular disease of the bone are a heterogenous group of disorders in which hereditary and environmental factors in combination with an altered immune response appear to play a causative and pathogenic role in its occurrence. Alkaline phosphatase (ALP) is an enzyme found in all tissues, with particularly high concentrations of ALP observed in the liver, bile ducts, placenta, and bone.Alkaline phosphatase is an orthophosphoric monoester phosphohydrolase catalyzing the hydrolysis of organic esters at alkaline pH, indicating that alkaline phosphatase is involved in fundamental biological processes.1 The present study envisages on identifying the specific electromorphic association of alkaline phosphatase with arthritides. Phenotyping of serum samples was carried out by PAGE (Polyacrylamide gel electrophoresis) following Davies (1964)2 protocol on 41 juvenile arthritis, 150 rheumatoid arthritis and 100 osteo arthritis apart from, 25 normal children and 100 adult healthy subjects. Phenotyping of alkaline phosphatase revealed an increase in preponderance of p+ and p++ phenotypes in juvenile, rheumatoid and osteo arthritic patients. However a significant association of these phenotypes was observed only with rheumatoid arthritis condition (c2:17.46). Similarly, a significant increase of p+ phenotypes in female rheumatoid arthritis patients was observed (c2:14.973), suggesting that the decrease in p° (tissue non specific) synthesis/secretion of alkaline phosphatase could be associated with decreased mineralization and ossification process in arthritis condition.INTRODUCTION Arthritides categorised as juvenile, rheumatoid arthritis and osteo arthritis, are a heterogeneous group of disorders, predominantly affecting the joints and causes inflammation of the synovial membrane leading to erosion & destruction of the joint cartilage. Heredity as well as environmental factors, in combination with humoral response may play a causative and pathogenic role in the aetiology of arthritides, with the common mode of inheritance reported to be multifactorial in nature. Juvenile arthritis is a condition that causes inflammation in one or more joints and begins before the age of 16. Rheumatoid arthritis, is an inflammatory disease in which the immune system attacks the tissues, particularly the joints & synovium, resulting in swelling, stiffness & loss of function in the joints and the age at onset was observed to be usually between 20-40 years.[3] Osteo arthritis is the most common form of arthritis in which a tilt in normal balance between cartilage synthesis and degradation is observed[4] with the incidence found to be increased between 40-70 years of age. Although alkaline phosphatase is found in many tissues, the highest concentrations are found in the liver, biliary tract epithelium, and bone. Alkaline phosphatase is a nonspecific phosphomonoesterase that hydrolyze phosphate monoesters and is found attached to the plasma membranes where extensive transport takes place, indicating that alkaline phosphatase is involved in fundamental biological processes.[1] Since it is found localized in the plasma membrane of the osteoblastic cells, its role in bone mineralization is justified.[5] The tissue specific alkaline phosphatase gene is found to be located on chromosome 2q34-37 while the tissue non-specific gene is assigned to 1p34-36.1 chromosomal region.[6] Three distinct isozymes p°, p+ and p++ of alkaline phosphatase encoded by three structural genes is reported with characteristic type of several tissues involved in its secretion like the bone/kidney, intestinal and placental types respectively. Since no information with regards to alkaline phosphatase and its electromorph association with arthritis is available, such a study is imperative which may help in risk prediction and in delineation of genetic heterogeneity of the condition. Therefore, the present study aims at identifying specific electromorph association of alkaline phosphatase in the etiology of Arthritides. MATERIAL AND METHODS The present study includes arthritides patients referred to out patient unit of orthopedic department at Andhra Vaidya Vidhan Parishad, King Koti, Hyderabad. Cases of juvenile arthritis (JA), rheumatoid arthritis (RA) and osteo arthritis (OA) referred for the first time and confirmed radiologically based on small and large joint involvement were considered. For comparative purposes, juvenile and adult healthy individuals matched for age and sex were considered from voluntary blood donors of various blood camps organized by Lion′s Club and dental checkup camps by schools in and around Hyderabad city. Blood samples from 41 juvenile, 150 rheumatoid, 100 osteo arthritic patients, 25 juvenile children and 125 healthy individuals matched for age and sex were collected for the serum analysis of alkaline phosphatase. 5ml of venous blood was collected from each patient/individual in sterilized vials, for obtaining serum samples. The samples were centrifuged at 2000rpm for about 10minutes and the clear supernatant serum from clotted blood was collected in eppendorff tubes and were analyzed for alkaline phosphatase phenotypes. A 7%, vertical slab PAGE gel was prepared in the ratio of 1:1:2 wherein 1 volume of each contained solutions of Tris-borate (hydroxy methyl) methylamine and Acryl amide/ bis acryl amide solution, and two volumes contained Ammonium per sulfate following Smithies et al[7] protocol. Later the unit was connected to the anodic and cathodic ends of the DC power supply, with the tank buffer being Tris borate (pH 9.5) diluted 1: 4 folds 30ml of the serum sample was mixed with a drop of bromophenol blue indicator and layered in each sample slot/well. The electrophoresis was carried at a constant current of 20mA for 1hour at 4oC until the indicator reached the other end of the gel. Later the gel was stained with a staining solution containing 2mg b naphtyl disodium phosphate and 1mg fast blue (BB) salt dissolved in 1ml location buffer of boric acid and magnesium chloride (pH 9.7). The gel was kept in the incubator maintained at 37oC until pink bands appeared and based on their eletrophoretic mobility and intensity of staining the phenotypes of alkaline phosphatase were identified as p°, p+ and p++ respectively. The phenotypic frequencies were computed and c2 test of analysis (2x2 contingency), Woolf′s test of relative association was carried out to interpret the results statistically.[8] RESULTS Table 1 presents the frequency distribution of alkaline phosphatase phenotypes in the control and disease groups. The difference of these phenotypes between juvenile arthritis and juvenile controls was statistically insignificant (c2 -3.509). A significant difference was noted in the of alkaline phosphatase phenotypes in rheumatoid arthritis condition (c2 -20.650; p<0.001) as compared to controls. Whereas no significant variation was observed between osteoarthritis and controls (c2 -1.424). To test for an association, relative risk estimates of alkaline phosphatase in control and juvenile arthritis group is computed and presented in [Table - 2]. The relative risk estimates were not found to vary with juvenile arthritis condition. The relative risk estimate of alkaline phosphatase phenotypes in rheumatoid arthritis in comparison to control group is presented in [Table - 3]. A significant association of alkaline phosphatase phenotypes was observed only with rheumatoid arthritis condition. The relative risk estimate of alkaline phosphatase phenotypes in osteo arthritis in comparison to the control group is presented in [Table - 4]. No significant variation in the phenotypic distribution of alkaline phosphatase was observed in osteo arthritic condition. [Table - 5] gives the frequency distribution of alkaline phosphatase phenotype with respect to sex in disease and control groups. Phenotypes of alkaline phosphatase did not seem to vary in juvenile arthritis though predominance of p+ and p++ phenotypes in female patiens (35.7% and 14.3% respectively) were observed when compared to the control group (22.2% and 11.1% respectively). Similarly p+ phenotypes were found to be predominant in male patients (53.0%) compared to male control subjects (25.0%). Predominance of p+ phenotype and decreased predisposition of p0 phenotypes in female patients of rheumatoid arthritis were found to be significantly associated (c2 : 14.973), while in male rheumatoid arthritis and osteo arthritis patients, an increased predisposition of p+ and p++ phenotypes was observed with the association being insignificant. DISCUSSION Alkaline phosphate (ALP), a phosphomonoester was examined for its isoenzyme variation in arthritides in the present study. An increased prevalence of p+ phenotypic individuals in juvenile arthritis (41.5%) compared to juvenile control groups (24.0%) was observed. Similarly, p+ and p++ phenotypes were found to be significantly higher in individuals of rheumatoid arthritis (c2 : 20.65) only indicating preponderance of intestinal component may predispose an individual to the disease condition and/or deficiency of p° phenotype of alkaline phophatase may contribute to a decrease in bone mineralization and bone formation processes.[9] Alternatively, individuals of p+ and p++ phenotypic individuals could be predisposed to increased risk to develop arthritides, indicating that the intestinal secretion/synthesis of alkaline phosphatase could be enhanced, as alkaline phosphatase is needed for the mineralization and ossification processes of the bone, which could be mediated by calcium. Further, the reduced alkaline phosphatase p° phenotypic frequency in the diseased condition may attribute to decreased series of tissue non specific (bone/kidney/liver) component confirming the decreased ossification process. Studies indicate that during adulthood, activity of alkaline phosphatase bone fraction is constant and no significant differences were observed between sexes, neither for bone nor for liver alkaline phosphatase activity.[10] However, alkaline phosphatase phenotypic distribution was found to be associated with predominance of intestinal component in our study, correlating the observation to decreased bone mineralization and ossification and an increased bone resorption. Hence, to maintain serum homeostasis of alkaline phosphatase, a simultaneous increase of intestinal component secretion of alkaline phosphatase can be observed, which is also found to correlate with the increase in p+/p++ phenotypes in rheumatoid arthritis patients. In conclusion, deficiency of alkaline phosphatase p° isoenzymes observed in arthritides confirms decreased bone mineralization and low bone formation in the disease process. Implication for future research Estimation of ALP levels and its individual components may be of relevance for drug discovery and clinical trials. ACKNOWLEDGEMENT We acknowledge the financial support from UGC- New Delhi.REFERENCES
Copyright 2004 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg04002t3.jpg] [hg04002t2.jpg] [hg04002t4.jpg] [hg04002t5.jpg] [hg04002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}