 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
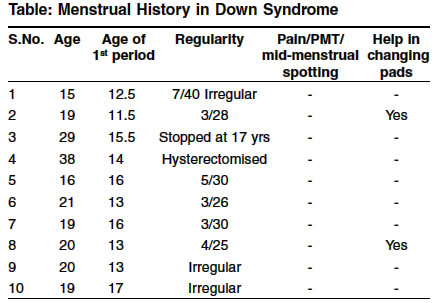
Indian Journal of Human Genetics, Vol. 10, No. 1, Jan-June, 2004, pp. 18-21 Original Article Menstrual history in women with down syndrome - A review Ranganath Priya , Rajangam Sayee Department of Anatomy, St. John's Medical College, Bangalore Code Number: hg04005 ABSTRACT The parents of 130 Down Syndrome (DS) females aged 15 to 40 years were requested to pen the information about the menstrual cycle details. Only 10 responded to the request. In view of the absence of information on DS in India regarding menstrual history, the present investigation has been undertaken. It has given the following observations: The axillary and pubic hair is present in most of the females. Most of them have a normal voice. As for the menstrual history, the age of onset of menstruation was at an average age of 15.5 years, the previous and the present menstrual history are normal in most of them. None of the females have pain during menstruation, premenstrual tension or mid menstrual pain or spotting. Most of them need help in changing sanitary pads. One has been hysterectomized. Hence, appropriate regular gynecological care is emphasized.INTRODUCTION At some point in their lives, many women experience some kind of menstrual disorder - heavy, painful, scanty, non-existent, or irregular menstrual flow. This is also true for women with Down Syndrome. Once the menses are established, usually within the first 6-18 months of menarche, most adolescents with DS have regular periods. The average age of the first period is usually between 11 and 13 years for this population, whereas it is typically between 10.2 and 11.2 years in the general population.[1] Rarick et al[2] have observed that their sample of girls with DS had normal growth rates. When they subdivided adolescents into two time periods (10-14 years and 15-18 years of age), they found that the girls had a later pubertal growth spurt than girls without disabilities. The maximum size of the growth spurt in adolescents with DS was 6.61 cm for girls compared to 7.8 cm for girls without disabilities. On an average, the growth spurt for both boys and girls with DS was found to be a year later than in adolescents without disabilities.[3] Taking these ideas into consideration, the present study has been attempted to find out the menstrual history of DS females and to analyze the difficulties that they and their family have faced. MATERIALS AND METHODS A detailed proforma containing information on menstrual history was mailed to the parents of the cytogenetically confirmed 130 DS females, aged between 15 to 40 years, attending the out patient department at the Division of Human Genetics, St. John′s Medical College, Bangalore. Self-addressed, stamped envelopes were also enclosed for their reply. RESULTS It is to be noted that only 10 DS families have responded. Twenty covers have been received stating that the addressee have left without forwarding addresses. The rest did not respond. By analyzing the proforma given by the parents of the DS females, the following facts were observed:Secondary sexual characteristics
Menstrual history
Family history The mothers of 8 females have regular periods whereas 2 have irregular periods.
DISCUSSION Limited information is available in the medical literature on the physical and sexual maturation of female adolescents with DS. Some of the early literature is based on studies conducted in institutions for people with mental retardation, and as on today, the results of those studies may not be applicable to adolescents with DS.[4] Secondary sexual characteristics: Bleyer[5] in 1937 has reported that the labia majora are frequently oversized and that the labia minora are enlarged and protruding. Such observations have not been made by Scola and Pueschel.[6] Shelley and Butterworth[7] have noted underdevelopment or absence of axillary apocrine glands as well as diminished axillary hair. Smith et al[8] have reported delayed development of axillary hair in females with DS. Menstrual history: The age of onset of menstruation and characteristics of the menstrual cycle have been studied by Bellone et al.[9] These investigators have found the average age of onset of the menstrual period to be 13.1 years in females with DS. They have also noted that the menstrual cycles occurred every 26-34 days in about two thirds of the study population. Menorrhagia (i.e., prolonged or excessive periods) and metrorrhagia (i.e., frequent and irregular periods) have been found to be the common presenting complaints in females with DS.[10],[11] More recently, Scola and Pueschel[6] have reported that the average onset of the first menstrual cycle in young females with DS was 12.6 years, compared to their sisters whose average menarche was at 12.1 years. In this study, of the 38 adolescent females with DS who had menstruated at least once, 29 were described as having regular menstrual cycles. The nine females with irregular cycles included three who had their first period in the preceding month, two who had spotted several times without an established pattern, and four who had very irregular patterns but a normal to heavy flow rate. Authors have also reported that the average length from the first day of the cycle to the first day of the next cycle varied from 22 days to 33 days. The menstrual flow lasted, on an average, 4 days. The amount of flow was described as normal for 22 females, heavy for 5 youngsters, and light for 2. The vast majority of young women with DS in this study did not require help with menstrual hygiene, and only 6 of the 29 females needed assistance at times with changing pads. Like all women, women with DS may have menstrual irregularities that require treatment, and have a chance of developing cervical, breast, or other cancers. In addition, they often require more counseling and guidance about menstrual hygiene, reproductive issues, and appropriate sexual behaviour. It is largely up to the parents to ensure that the teenager receives the gynecologic care she needs. This seems to be a daunting prospect, but with the support of a gynecologist, the parent could teach the daughter to take responsibility for her own care. Most women with DS are quite capable of good menstrual hygiene and of looking after their own reproductive health.[12] Most young women with DS have regular monthly cycle. The regular menstrual cycle begins after initial irregular bleeding episodes that usually follow the start of growth of hair in armpit and pubis. The average age of ′menarche′, or the age when menses begins, has been falling steadily in America over the past 25 years. It is now about 10.5 to 11.2 years of age. Young women with DS also follow a similar pattern, with menarche ranging from 11 to 13 years in some surveys. As with other physical traits, women with DS may show a wide range of characteristics, with some having delay in menarche beyond age 18 with no identifiable cause other than DS. However, the majority of young women with DS have regular menstrual cycles. Menstrual hygiene is often a major concern for families, but worries about menses before they begin are typically worse than warranted. Most young women with DS can manage their menstrual cycles quite successfully with proper training. Some may need medications to help control menstrual flow as a part of their hygiene training 1.[2] Aetiology of menstrual disorders: The menstrual disorders could result from a variety of causes, including certain disorders that may be associated with DS. Some of the more common causes of menstrual disorders are thyroid abnormalities, brain tumors, CNS disorders, pelvic tumor, poor nutrition, endometrial cancer. Causes of amenorrhea include thyroid disease which is common in DS.[13] Thyroid disorders occur more commonly in people with DS than in the general population. Many tend to be overweight[14] which could be associated with irregular and heavy periods. Family planning measures: It has been opined that intrauterine devices are usually not an optimal contraceptive choice for females with DS. The devices may be associated with heavier vaginal bleeding (adding to any problems associated with menstrual hygiene), increased dysmenorrhea, and risk for pelvic infections.[4] There is fear that a young woman with DS will either enter into a sexual relationship or be sexually abused and thus exposed to an unwanted pregnancy. Because of this concern many of these young women in the past have been sterilized by bilateral tubal ligation or hysterectomy. However, oral contraceptive agents, Depomedroxyprogesterone, and the levonorgestrel implant system have been found to be relatively safe and effective.[1] In very rare instances, hysterectomy may be considered to help a woman with DS manage her menstrual hygiene. For example, a woman with heavy menses flow and severe behavior management problems may be considered for a hysterectomy. However, these are very high-risk alternatives. Surgical risks include hemorrhage (1-3%), aspiration pneumonia (1-5%), deep venous thrombophlebitis with pulmonary embolus, damage to bowel-bladder-ureter (1-2%), infection (5%), and even death. Because of these risks, this procedure should only be a last resort.[12] In the present study, the observed secondary sexual characteristics, especially distribution of axillary and pubic hair is found to be as reported by Shelley and Butterworth.[7] Smith et al[8] and Scola and Pueschel.[6] The mean age of menarche in our study group is 15.5 years. In literature, the reported mean age ranged from 11 to 13.1 years.[9],[6],[12] The late onset of menarche in the present study could be attributed to race, ethnicity, sample size, sexual awareness, nutrition and small build. The irregularity in the cycle such as duration of flow, pain and help required during menstruation are found to be more or less as reported in literature. It may be noted that one patient tending towards premature ovarian failure needs further follow-up. One of the cases has undergone hysterectomy possibly because of parental anxiety towards sexual abuse, unwanted pregnancy and the need for parental help. [Table - 1] Thus, routine gynecologic care is essential for the physical, mental, and emotional health of the adolescent with DS. The concerns and problems noted in this group are often the same as those seen in young women without DS. Helping to prepare parents and caregivers for this complex stage of life in DS is as important as counseling the normal adolescent. REFERENCES
Copyright 2004 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg04005t1.jpg] |
| |||||||||

{kind=link}