 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
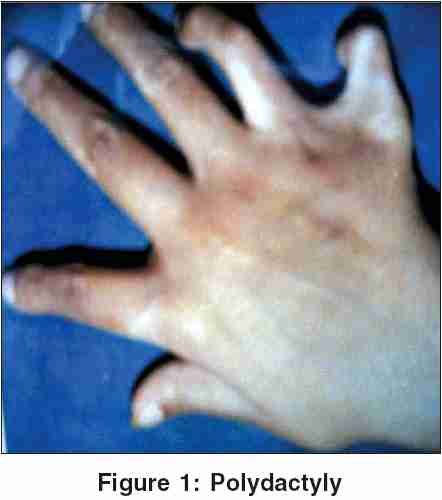
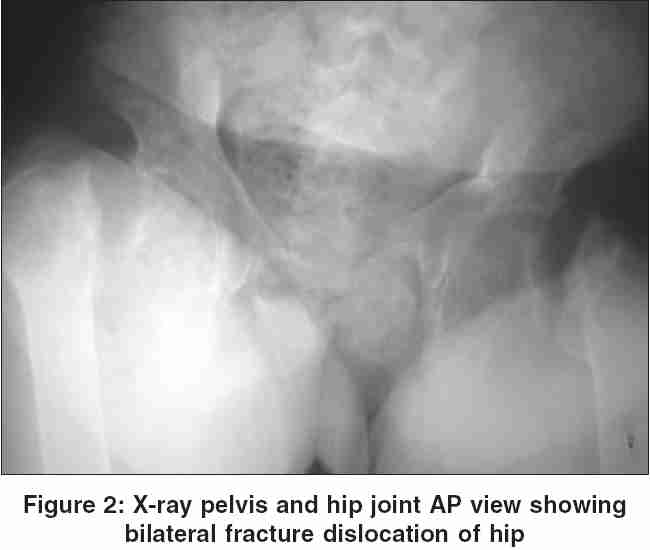
Indian Journal of Human Genetics, Vol. 11, No. 3, September-December, 2005, pp. 159-160 Letter To Editor A rare presentation of Bardet-Biedl syndrome with renal failure, severe osteodystrophy and multiple fractures Gupta S, Goel D, Singhal A Himalayan Institute of Medical Sciences, Swami Ram Nagar, Dehradun (UA), India Code Number: hg05032 Sir, Bardet-Biedl syndrome (BBS) is a rare (1: 160000 population) heterogeneous, autosomal recessive disorder characterized by polydactyly, obesity, mental retardation, hypogonadism and renal failure. This is also called Laurence- Moon-Bardet-Biedl syndrome (LMBBS), but different from Laurence- Moon-Biedl syndrome (LMBS). This entity came into picture when George Bardet done his MD thesis on " Hypothalamic obesity" under Louis Pasteur. He noticed number of cases with unusual features in particular hexadectyly, retinitis pigmentosa and obesity. This syndrome needs either four primary or three primary plus two secondary features for the diagnosis. Primary features -Red cone dystrophy, Polydactyly, Obesity, Learning disability, Hypogonadism in male, renal abnormalities Secondary features Speech disorder, Brachydatyly, Developmental delay, Polyuria/ polydipsia, Ataxia, Poor coordination/ clumpsiness, Diabetes mellitus, Left ventricular hypertrophy, Hepatic fibrosis, Spasticity[1]. BBS is an autosomal recessive, genetically heterogeneous condition, with four loci mapped till date. These are BBS1 (11q13), BBS2 (16q22), BBS3 (3p13), and BBS4 (15q21). BBS1 involved in 45% of affected white families and BBS4 is next most common. But there are several families from Middle East and Asia, which do not show any of the known linkage[2]. BBS is distinguished from the much rarer Laurence-Moon syndrome in which retinal pigmentry degeneration, mental retardation and hypogonadism occur with progressive spastic paraparesis and distal muscle weakness but without polydactyly. We report a case of BBS with renal failure and unusual features of renal osteodystrophy. A 20 years old girl presented to us with history of progressive weakness of both lower limbs for the last two years. She was full term normal delivered, born as a result of non-consanguineous marriage. The motor and mental milestones were normal. She was evaluated for night blindness the age of 5 years, which was followed by gradual loss of vision in both eyes. She was having poor physical growth and primary ammenorhoea.As she grew up there was difficulty in walking. She had non-united fracture of left tibia 18 months back on a trivial trauma (Pathological fracture). She gradually lost weight and developed slowly progressive painful weakness of both lower limbs. She used to lie down with flexion attitude and developed bilateral contractures of knee joints. She was a moderately built, short stature girl with a blood pressure was 130/80mmHg, mild pallor, ankle edema, strabismus in right eye, polydactyly [Figure1], scoliosis of spine towards left side and the movements at both the hip joints were restricted due to pain. Fundoscopy showed retinitis pigmentosa, visual acuity was markedly reduced (only hand movements at two feet). Hemoglobin 11.9 gm%, total leukocyte count 8920 / cmm (P76, L 23 E 01), ESR =50 mm in first hour, platlet count 2.8 lacs / cmm, RBCs=normocytic, normochromic. Urine analysis: Alb. Traces, sugar =nil, microscopy was normal. Serum biochemisty: Creatinine = 3.0 mg%, K+ = 3.59 mmol/L, inorganic phosphorus = 2.8mg%, calcium = 4.6 mg%, blood sugar = 85 mg%, albumin = 3.6 gm%, alkaline phosphates = 355 IU / L, serum intact-PTH = 538 pg / ml, X-ray chest PA view showed kyphoscoliosis with hypoplasia of left lung and bilateral fractures of neck of humerus. X-ray pelvis AP view revealed bilateral fracture dislocation of hip [Figure - 2], with fracture of pubic symphysis and callus formation. X-ray cervical spine showed fracture at the angle of left mandible. USG - KUB revealed bilateral hypo plastic kidneys with normal cortico-medullary differentiation. This case has all primary features of BBS. This patient had predominant changes in skeletal system as bilateral hip and other fractures, Kypho-scoliosis, and secondary hyperparathyroidism. This all findings can be explained on the basis of renal osteodystrophy with advance renal failure. Various causes has been described for rare association of bilateral hip fracture in renal failure, which includes, patients on chronic hemodialysis, avascular necrosis in post - transplanted patients, due to seizure, amyloidosis, fluorosis and aluminium toxicity during dialysis[3]. But none of the factor was positive in our patient. Several patients had marked joint laxity with multiple dislocations of shoulder and patella in BBS. But hip dislocation is not being described to our best knowledge. This case has given us the insight of this rare condition with some new findings. References
Copyright 2005 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg05032f1.jpg] [hg05032f2.jpg] |
| |||||||||

{kind=link}
{kind=link}