 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
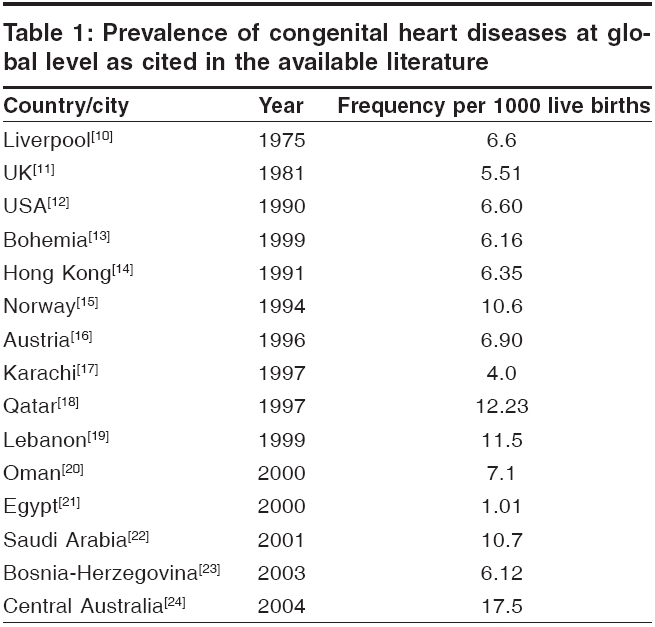
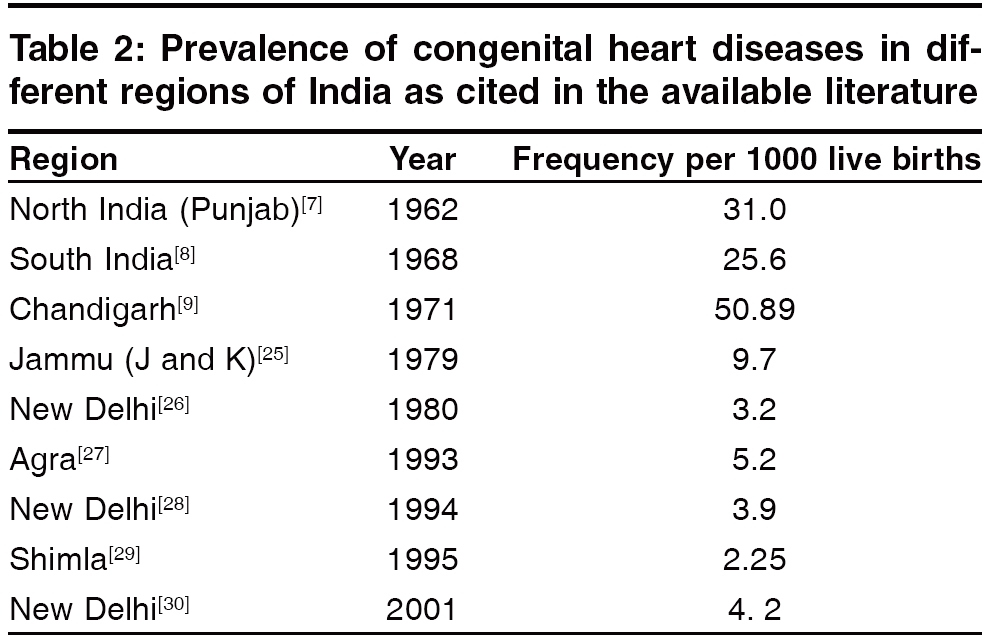
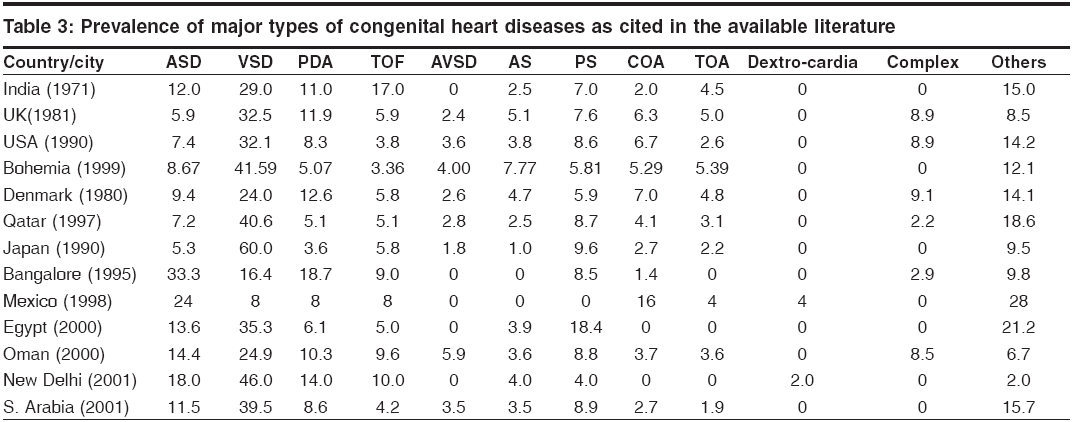
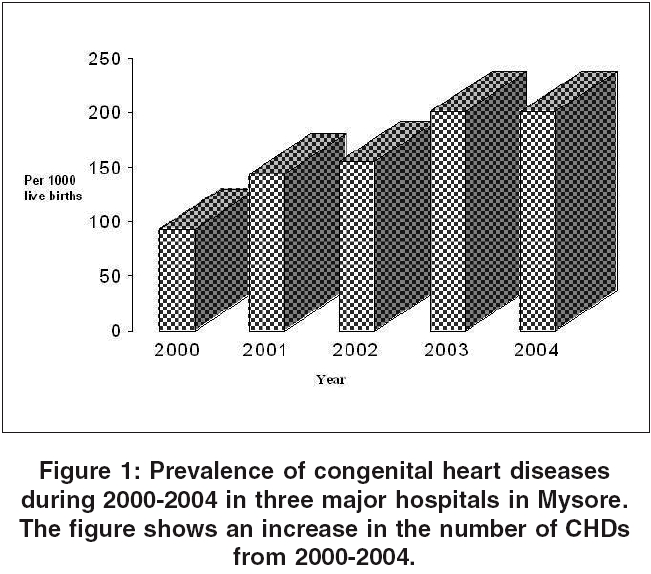
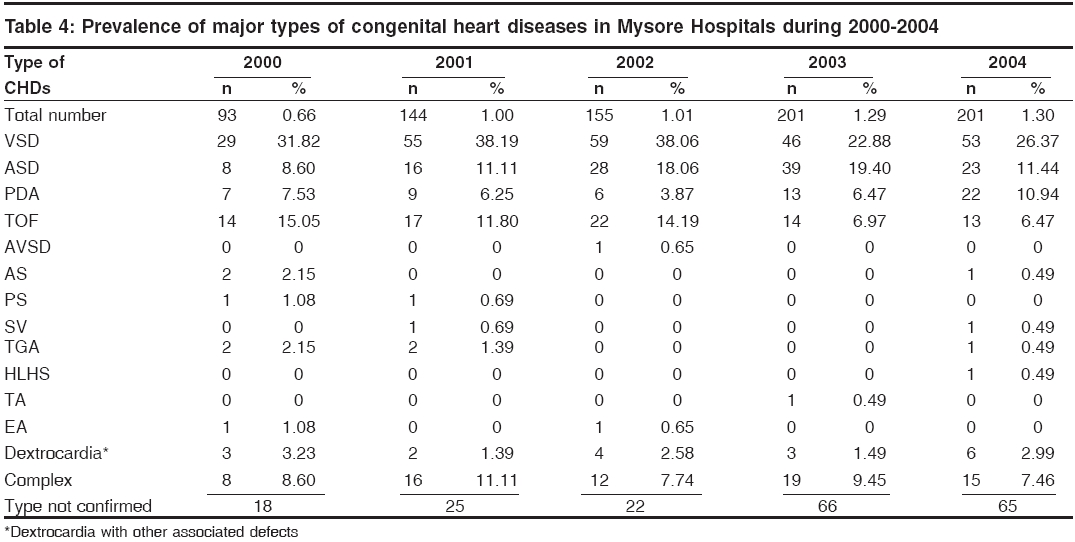
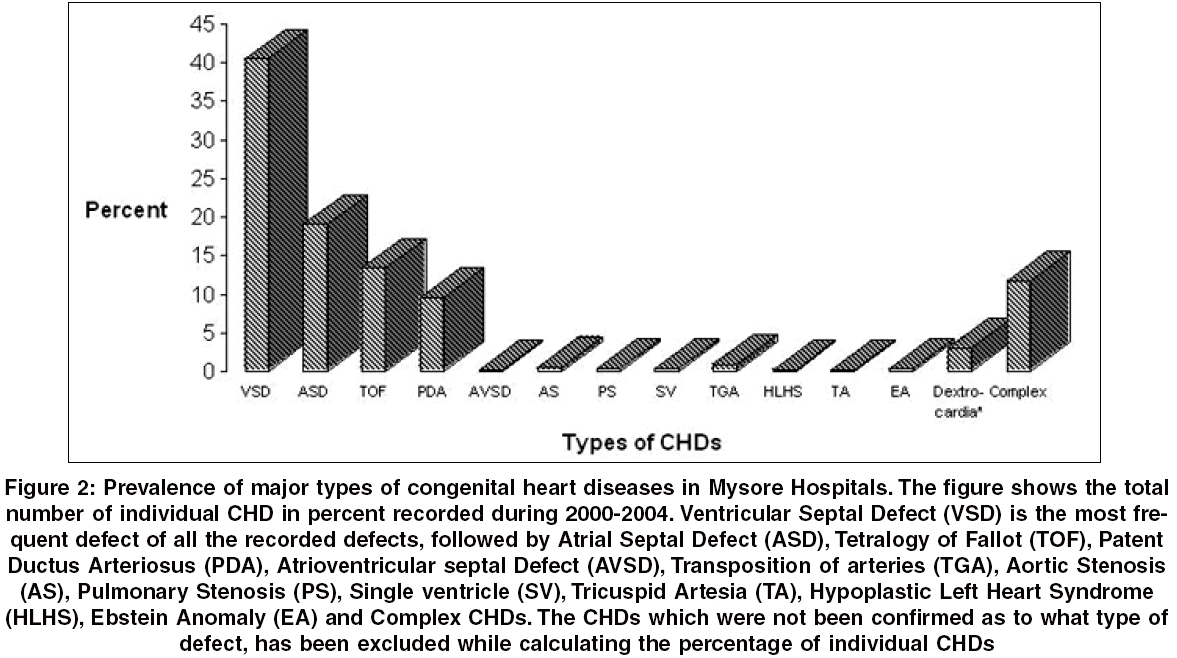
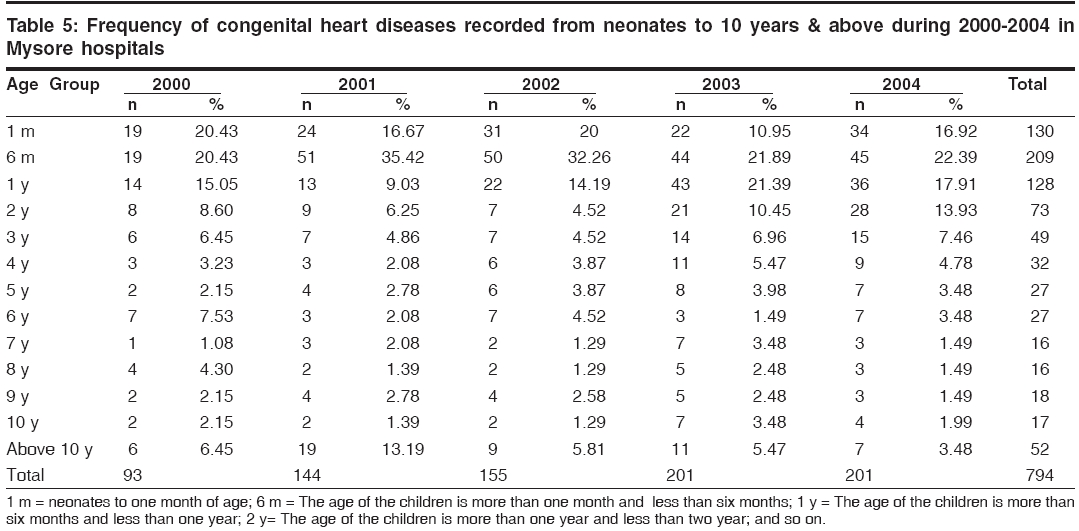
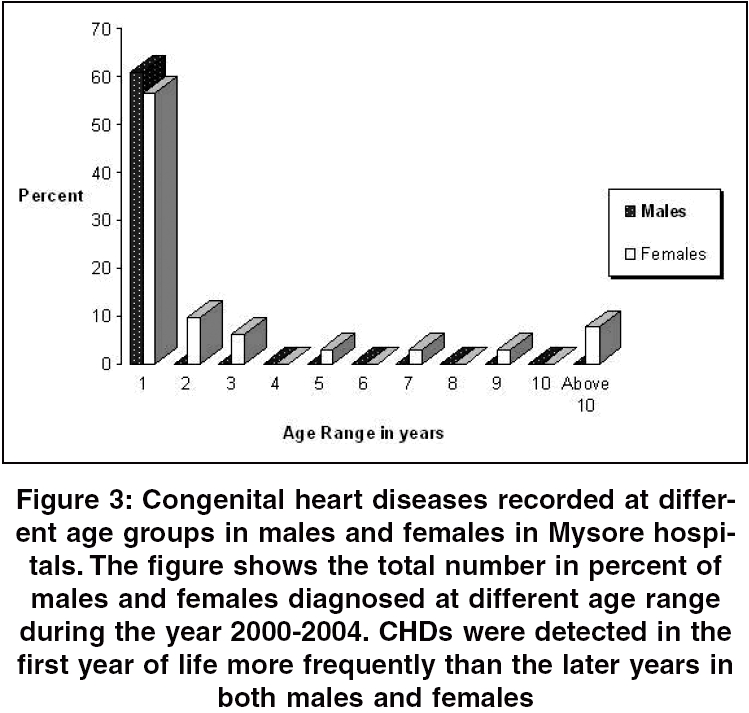
Indian Journal of Human Genetics, Vol. 12, No. 1, January-April, 2006, pp. 11-16 Original Communication Prevalence of congenital heart diseases in Mysore R. Smitha1 , S. C. Karat2 , D. Narayanappa3 , B. Krishnamurthy4 , S. N. Prasanth3 , N. B. Ramachandra1 1 Human Genetics Laboratory, Department of Studies in Zoology, University of Mysore, Manasagangothri, Mysore - 570006, 2 Department of Pediatrics, CSI Holdsworth Memorial Hospital, Mysore, 3 Department of Pediatrics, JSS Hospital, Mysore, 4 Department of Pediatrics, Cheluvamba Hospital, Mysore Correspondence Address:Department of Studies in Zoology, University of Mysore, Manasagangothri, Mysore - 570006, rnallur@sancharnet.in Code Number: hg06003 Abstract Background: Prevalence studies on Congenital heart Diseases (CHDs) have been done several times world wide and such studies are very limited in Indian populations. A few earlier studies in India have reported an increased prevalence of CHDs ranging from 2.25 to 50.89 per 1000 live births.Aims and Objective: To study the prevalence of congenital heart diseases in Indian population. Materials and Methods: Data on the prevalence of CHDs were collected and analyzed from the three major hospitals of Mysore, Cheluvamba Hospital, CSI Holdsworth Memorial Hospital and J.S.S Hospital from the year 2000 to 2004. Results: The prevalence of CHDs for five years in Mysore hospitals ranges from 6.6 to 13.06 per 1000 live births. The most frequent type of CHD was found to be VSD (40.47%) followed by ASD (19.06%), TOF (13.38%) and PDA (9.53%). It is clear that the maximum CHDs were detected in the first year of life when compared to the later years of life. The prevalence of CHDs in Mysore is increasing from 2000 to 2004 which might be due to the improvement of diagnosis, attention or awareness among the medical authorities on the disease. Conclusion: The prevalence of CHDs in Mysore is not very high as reported in other parts of the country, however; it is an important disease which needs an immediate medical attention. Keywords: Congenital heart diseases, epidemiology, Mysore, prevalence, ventricular septal defect Introduction Congenital heart diseases (CHDs) are the malformation of the heart or the large blood vessels associated with the heart, affecting various parts or function. It is one of the leading causes of mortality in the first year of life.[1],[2],[3] CHDs are the common single group of abnormalities accounting for about 30% of the total congenital abnormalities.[1] It has been estimated that some types of CHDs can be related to the defects in the chromosome, gene or environmental factors.[4] In ~90% of the CHD cases, there is no identifiable cause that can be attributed as multifactorial defects. The majority of these structural abnormalities occur as isolated malformation in most patients, but about 33% have associated anomalies.[5] According to the Merck Manual of Diagnosis[6] the different types of CHDs are Atrial Septal Defect (ASD), Ventricular Septal Defect (VSD), Tetralogy of Fallot (TOF), Patent Ductus Arteriosus (PDA), Pulmonary Stenosis (PS), Aortic Stenosis (AS), Coarctation of Aorta (COA) and Atrioventricular Septal Defect (AVSD) which accounts for 85% of all CHDs. The remaining 15% of rare and complex CHDs are Persistent Truncus Arteriosus (PTA), Tricuspid Atresia (TA), Total Anomalous Pulmonary Venous Connection (TAPVC), Hypoplastic Left Heart Syndrome (HLHS), Double Outlet Right Ventricle (DORV), Single Ventricle (SV), Ebstein Anomaly (EA) and Dextrocardia. Prevalence studies on CHDs have been done several times world wide. Although it is a common disease, a few studies on the prevalence of CHDs in India have been reported, of which, prevalence of CHDs in Chandigarh (5%), Punjab (3%) and South India (2.5%) are higher than other parts of the world.[7],[8],[9] In view of this, we report the prevalence of CHDs for 5 years among the patients in different hospitals of Mysore. Materials and Methods The present investigation was conducted in Mysore from the year 2000 to 2004. Data on the prevalence of CHDs were collected and analyzed from the three major hospitals, Cheluvamba Hospital, CSI Holdsworth Memorial Hospital and J.S.S Hospital. These hospitals receive major number of children as patients which also includes patients referred by other hospitals from in and around Mysore. These hospitals are easily accessible to all the city inmates as well as, to the inmates of neighbouring districts and are affordable to the common man. The subjects in the present study included pediatric live births and inpatients that had been examined for various illnesses in the hospital by the pediatricians. The source of information was the medical and echocardiography records at these hospitals. The suspected CHD patients who showed symptoms like poor feeding, failure to thrive, respiratory problem, discrepancy in pulse, cyanosis, heart murmur, abnormal chest X-ray, or strong family history had been subjected by the authors for further clinical diagnosis, extensive X-ray analysis, ECG and echocardiography examination for the conformation of the CHDs. Care had been taken to avoid duplication of the cases in the same hospital or the cross over to other hospitals in Mysore during the study period. Prevalence, age and sex specific frequency of all kinds of CHDs were computed. The different types of CHDs considered for the present investigation are: Ventricular septal defect (VSD), Atrial septal defect (ASD), Tetralogy of Fallot (TOF), Patent Ductus Arteriosus (PDA), Pulmonary Stenosis (PS), Aortic Stenosis (AS), Transposition of Great Arteries (TGA), Atrioventricular septal defect (AVSD), Dextrocardia, Tricuspid Artesia (TA), Hypoplastic Left Heart Syndrome (HLHS), Single ventricle (SV), Ebstein anomaly (EA) and Complex CHDs (various types of CHDs existing together including rare type of CHDs). Exclusion criteria included CHDs with associated syndromes, since the present study was to know the prevalence of isolated CHDs in Mysore. Results At the global level excluding India, population based epidemiological studies on CHDs have indicated a prevalence ranging from 1.01 (Egypt) to 17.5 (Central Australia) per 1000 live births [Table - 1].[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24] [Table - 2] shows the prevalence of CHDs in India.[7],[8],[9],[25],[26],[27],[28],[29],[30] Studies in Chandigarh showed the maximum prevalence of 50.89 per 1000 live births[9] whereas studies in Shimla showed the minimum of 2.25 per 1000 live births.[29] [Table - 3] presents the prevalence of different types of CHDs world wide in which VSD is found to be the most prevalent type of defect.[8],[20],[21],[22],[23],[24],[31],[32],[33],[[34] The present investigation in Mysore, from 2000 to 2004, revealed a mean prevalence of 10.65 per 1000 live births of the total 74,589 inpatients and live births with a yearly prevalence varying from 6.6 to 13.06 per 1000 live births [Figure - 1]. [Table - 4] displays the total number of CHDs and different types of CHDs recorded in the present study with their prevalence. The most frequent type of CHD was found to be VSD (242 patients) with a prevalence of 40.47% of the total CHDs recorded. The other frequent defects were found to be ASD (114 patients) with a prevalence of 19.06% followed by TOF with 13.38% (80 patients) and PDA with 9.53% (57 patients). Less frequent types of CHDs were AVSD, AS, PS, TGA, SV, HLHS, TA, EA, Dextrocardia and complex CHDs [Figure - 2]. [Table - 5] reveals the age when the CHDs were detected in the patients. It is clear that the maximum CHDs were detected in the first year of life when compared to the later years of life [Figure - 3]. Discussion The recent exponential increase in the knowledge of genetics has revolutionized the understanding of CHDs during the past few decades.[35] India alone has one sixth share of the world population, which is a suitable place to generate meaningful data on the prevalence of CHDs. Therefore the present work has been undertaken to understand the prevalence of CHDs in Mysore from the year 2000-2004. The analysis revealed a frequency of 10.65 per 1000 live births which is contradicting to the high prevalence of CHDs reported earlier in India. One of the explanations for the wide variation between the prevalence of CHDs could be the result of different methodologies used in various studies, as well as the variations in the ethnic occurrence and regional differences. The most frequent type of CHD was found to be VSD which is in accordance with other studies. The frequency of the rare types of CHDs like AVSD, AS, PS, TGA, SV, HLHS, TA, EA, Dextrocardia was less when compared to the western data but similar to other Indian studies.[28],[31],[32] This could be due to the severity of the defects which might have lead to the death of the patients before accessing the medical facilities. This might also be due to racial and genetic factors in different populations. Of the total CHDs a few cases which were clinically diagnosed as CHDs could not be categorized into their respective types due to lack of echocardiography report. It was found that maximum CHDs were detected in the first year of life when compared to the later years of life. The prevalence of CHDs in Mysore is increasing from 2000 to 2004 [Figure - 1] which might be due to the improvement of diagnosis, attention or awareness among the medical authorities on the disease. Missing of the CHD patients was avoided to the maximum as these three hospitals are the major and the largest hospitals which are easily reached by the common man. However, inevitably some cases would have escaped detection and referral which includes neonates, especially born at home who die without medical attention which can be considered as negligible. The present findings indicate that (a) prevalence of CHDs in Mysore is not as high as the prevalence reported by other Indian studies, (b) however; it is a serious problem, which requires immediate attention for the improvement of diagnostic and therapeutic facilities which is accessible to the common man. Acknowledgment We would like to acknowledge the in-charge and the staff of Medical Record Section of Cheluvamba Hospital, CSI Holdsworth Memorial Hospital and J.S.S. Hospital who have provided with the necessary information to conduct the present study. We thank University of Mysore for giving us (SR) an opportunity to carry out our research activities and others Doctors and PG students of all the three hospitals who have rendered there help for this study.References
Copyright 2006 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg06003f2.jpg] [hg06003t3.jpg] [hg06003f1.jpg] [hg06003f3.jpg] [hg06003t1.jpg] [hg06003t4.jpg] [hg06003t5.jpg] [hg06003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}