 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
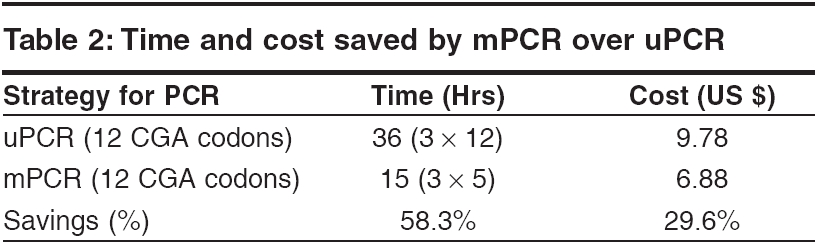
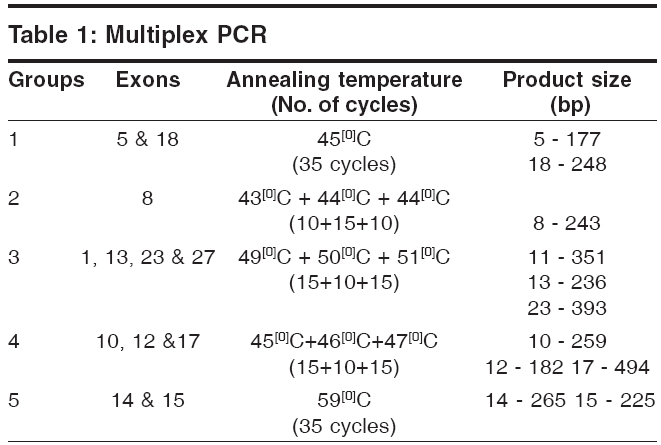
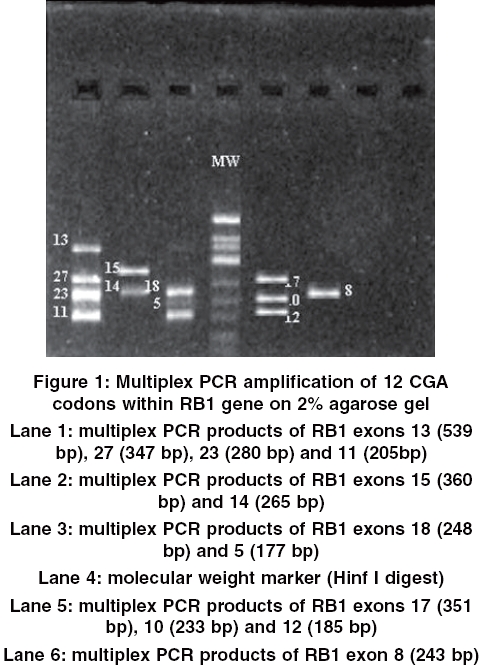
Indian Journal of Human Genetics, Vol. 12, No. 1, January-April, 2006, pp. 34-38 Original Communication CGA codons multiplex PCR in rapid diagnosis of retinoblastoma Gandra Mamatha, Biju Joseph, Mahesh Palanivelu Shanmugam*, Govindasamy Kumaramanickavel SN ONGC, Departments of Genetics and Molecular Biology, *Dept of Medical Retina, Medical and Vision Research Foundations Code Number: hg06007 Abstract Background: Multiplex polymerase chain reaction allows amplification of multiple target sequences of a genome under identical conditions in a single tube. This "one-shot" polymerase chain reaction detection is time and cost effective when large or multiple genes, with many target fragments are investigated. This is applicable for retinoblastoma susceptibility gene having 27 exons with recurrent mutations reported at most of the 12 CGA codons.Materials and Methods: Multiplex polymerase chain reaction assay for the amplification of 12 CGA codons, which constitutes about 50 % of retinoblastoma susceptibility gene mutations has been designed. The time and cost (includes only reagent cost) involved in both multiplex and uniplex polymerase chain reaction was also calculated. Results: Twelve CGA codons were multiplexed in 5 instead of 12 uniplex polymerase chain reactions, which took 36 hours and 9.78 US$ whereas multiplex polymerase chain reaction took 15 hours and 6.88 US$. Multiplex polymerase chain reaction method saved 58.3% of time and 29.6% of cost over uniplex polymerase chain reaction. Conclusion: Saving time by more than half and cost by nearly a third would help clinicians and geneticists while counseling retinoblastoma patients. Keywords: CGA codons, multiplex polymerase chain reaction, retinoblastoma, RB1 gene and rapid diagnosis. Introduction Retinoblastoma is a rare tumor that arises when both RB1 gene alleles are mutated. The developing retina has 4 x 10 6 cells, but only about 1 in 10 6 cells actually give rise to a tumor cell. Mutations in RB1 usually result in disruption of the protein product and cause retinoblastoma.[1],[2] One of the major goals in treatment of patients with retinoblastoma is early detection of retinoblastoma that helps in saving the vision in the affected eye. Despite the use of modern molecular techniques, there have been several obstacles to achieve the goal, because the retinoblastoma gene is very large and mutations occur throughout the gene with no single ′hot spot′.[3] Five to 8 percentof mutations in RB1 gene can be observed cytogenetically, which includes predominantly deletions but rarely insertions and translocations.[3] Remaining alterations are submicroscopic, which includes nonsense mutations, frame-shift mutations, missense mutations, in frame deletions, intron nucleotide change (alters splicing), loss of heterozygosity, or methylation of the promoter region. From various reports throughout the world it is found that in DNA mutations, non-sense and frame-shift mutations occur in 78% of retinoblastoma patients, intronic changes in 12% of patients, missense and small in-frame deletions in 8% of patients and nucleotide changes in the promoter region in 2% of patients.[4] Non-sense and frame-shift mutations result in premature termination of translation resulting in a truncated protein product, which cannot regulate the cell cycle. These mutations are more disruptive to protein function than other types of mutations.[4],[5] Cowell et al[6] has shown that the most common point mutation in the RB1 gene in retinoblastoma tumors is C->T transition and majority of these occur in CGA codons. As a result of this mutation, a TGA stop codon is generated directly which has been predicted to result in the absence of a functional protein. Fourteen CGA codons in the RB1 gene has been analysed for mutations in 113 patients with bilateral retinoblastoma. Six of these sites, C->T mutations in CGA codons alter a restriction enzyme site, which makes their identification relatively straightforward.[6] As majority of single base substitutions (76%) in RB1 gene are recurrent CpG transitions at 12 of the 15 CGA codons within the open reading frame,[4],[7] they can be identified by a relatively quick survey of the CGA codons. A mPCR (multiplex polymerase chain reaction) method for the amplification of 12 CGA codons of RB1 gene was designed, that allows rapid identification of RB1 mutations. The main advantage of mPCR is speed of analysis followed by economy on sample and reagents than uPCR (uniplex polymerase chain reaction) performed; less Taq polymerase, dNTPs and buffer; consumables including DNA. Simplicity of the method and sensitivity of the detection adds to the advantages of mPCR. According to this principle, we designed an extensive mPCR reaction for 12 CGA codons within RB1. Using this approach, we were able to save both time and cost. Materials and Methods The laboratory technique includes DNA extraction and multiplex PCR followed by 2% agarose gel electrophoresis. DNA Extraction Uniplex PCR Multiplex PCR For all amplifications 20 μl reaction mixture was prepared using 100 ng of genomic DNA, 4 pM of all primers, 3 μl dNTPs (40 nM), 4 μl PCR buffer and 0.6 U of Taq DNA polymerase. The PCR was carried out in the thermal cycler-PE 2700. The amplified products were separated on 2% agarose gel electrophoresis, captured by gel documentation system ImageMaster® VDS, Pharmacia Biotech using the Liscap software and analysed using Image master Total lab gel documentation system . The time and reagents consumed for uniplex and multiplex PCR was calculated. Results Uniplex PCR Multiplex PCR Discussion Recognition of the retinoblastoma gene and the technology to identify point mutations within will make it possible to offer antenatal diagnosis to an increasing number of patients. These advances at the molecular level will help to determine whether a new mutation is of somatic or germinal origin and thereby identify gene carriers. uPCR strategies are useful for mutational screening of small genes or genes with mutational hotspots. But these strategies will not be cost or labour efficient when large or multiple genes, with many target sequences are involved. In addition, such an approach is limited by sample quantity. Considerable saving of reagents, time and effort can be achieved by simultaneously amplifying multiple sequences in a single reaction, a process referred to as mPCR. The large size of the RB1 gene - 180 kb with an open reading frame of 2.7 kb and lack of mutation hotspots necessitates a mPCR based strategy in developing rapid DNA based diagnostic services for retinoblastoma. At the vitreous and retina department, Sankara Nethralaya, on an average 75 retinoblastoma patients are seen in a year. Nearly half of these families are one-child families.[8] A rapid molecular diagnostic method for retinoblastoma susceptibility gene will be useful for these families in taking a decision about having another child. Du and Gallie used quantitative fluorescent mPCR for mutational screening of RB1 gene and detected mutations in 50% of retinoblastoma patients screened.[9] In a study of pituitary tumours, mPCR was used for identification of homozygous deletion of exons 20-24 of RB1 gene from pituitary tumour DNA that failed to express retinoblastoma protein.[10] Lohmann et al analysed DNA from peripheral blood of 24 unrelated bilateral retinoblastoma patients without gross structural abnormalities by mPCR and polyacrylamide gel electrophoresis.[11] Screening of 26% of the RB1 coding region identified germline mutations 3 out of 24 bilateral retinoblastoma patients. mPCR followed by heteroduplex analysis and sequencing has been used as an efficient screening method for retinoblastoma.[12] RB1 gene is composed of 27 exons with no mutation hotspots. But majority of single base substitutions (76%) in RB1 gene are recurrent CpG transitions at 12 of the 15 CGA codons within the open reading frame (in the exons 8 (2 sites), 10, 11, 13, 14 (2 sites), 15, 17 (2 sites), 18 and 23) of RB1 gene.[3],[7] It is assumed that mPCR strategy for the CGA containing exons will offer an advantage for the rapid mutational screening and characterization of the mutational spectra of RB1 gene in retinoblastoma patients with considerable savings in time and reagents. Hence, based on diagnostic importance of the disease we designed mPCR method for the amplification of 12 CGA codons (exon 5, 8, 10 - 15,17,18, 23 and 27) as more than 50% of the RB1 gene mutations are reported in them. Initially the 12 exons of RB1 gene were PCR amplified in individual reactions. For mPCR, 12 CGA codons were separated in to five groups based on product size and annealing temperature at which PCR for individual exon has been standardized. Each group includes exons with nearby annealing temperature but with different product size. Parameters like annealing temperature, number of cycles were varied to obtain amplified products with high yield. The optimization of mPCR posed several difficulties. The presenceof more than one primer pair in the mPCR increases thechance of obtaining spurious amplification products, primarilybecause of the formation of primer dimers.[13] These nonspecificproducts may be amplified more efficiently than the desired target, consuming reaction components and producing impaired rates ofannealing and extension. To overcome the problem of non-specific amplification we initially altered PCR components such as PCR buffer constituents, dNTPs and enzyme concentrations overthose reported for most uniplex PCRs but there was no improvement in the yield, later when the annealing temperature was increased to one degree above the actual temperature at which uniplex PCR has been standardized for an individual exon, specific bands were obtained without any non-specific amplification. The CGA codon containing exons were multiplexed in five reactions [Table - 2], [Figure - 1] thus saving 21 hours (58.3 %) of PCR time. The cost savings involved in CGA codon mPCR is 2.9 US$ (29.6 %). Our calculations were based on the assumption that the time for one PCR run was 3 hours and only the reagent cost is included. In this way time for amplifying 12 exons in individual reactions were 36 hours. The multiplexed strategy enabled us to save 21 hours by amplifying twelve exons in five reactions. The amplification of exons 11, 13, 23 and 27 in the same PCR run saved 9 hours. Exons 10, 12 and 17 were amplified at 45oC+46oC+47oC in individual reactions saving 6 hours (exon 8 could not be multiplexed because the product size and annealing temperature did not fit in to any of the group). During the last decade, a number of studies have demonstrated the practicality of identifying RB1 gene mutations using mPCR. As per our knowledge, this is for the first time mPCR method has been optimized for CGA codons of RB1 gene; the purpose of our study is to facilitate rapid identification of RB1 mutations. We first screen CGA codons, which have 40-50% of mutations; if no mutation is detected then rest of the exons within the RB1 gene will be screened. Optimization of mPCRs that are designed for simultaneousamplification of multiple targets may prove beneficial for the RB1 diagnostics, which could have implications in genetic counselling. Acknowledgements We acknowledge the Department of Bio-technology, Government of India for their funding for the project titled ′"Developing DNA diagnostic methods for retinoblastoma and its application in genotype - phenotype correlation". Ref No. (BT/PR 1607/Med / 09/250/99(HG).References
Copyright 2006 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg06007t1.jpg] [hg06007f1.jpg] [hg06007t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}