 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
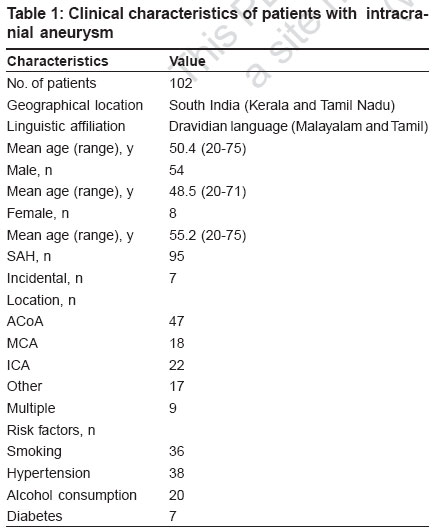
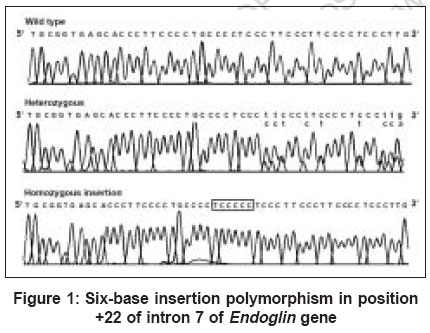
Indian Journal of Human Genetics, Vol. 12, No. 3, September-December, 2006, pp. 111-115 Original Communications Lack of association of Endoglin insertion polymorphism in intracranial aneurysm in South Indian population Koshy LindaV, Easwer HV, Bhattacharya RN, Banerjee Moinak Human Molecular Genetics Laboratory, Rajiv Gandhi Centre for Biotechnology, Thiruvananthapuram Code Number: hg06020 Abstract Background : Endoglin , is a component of transforming growth factor-β complex. It is involved in vascular development and structural maintenance of the vessel wall. Conflicting reports on the association of a six base insertion polymorphism in intron 7 of the endoglin gene in intracranial aneurysms (IA) have been reported earlier.Materials and Methods: A case-control study was designed to compare 102 South Indian patients with intracranial saccular aneurysms and 118 ethnically and geographically matched healthy controls. The frequency of the six base insertion polymorphism was assessed by heteroduplex analysis followed by direct sequencing. Results:Insertion allele count was 39 (19.1%) of 204 alleles in the patient group and 42 (17.8%) of 236 alleles in the control group. The INS allele frequency was similar to the frequency in Caucasian population, but it was significantly lower than the Japanese population ( P =0.01). There was also no relationship of this polymorphism in patients with single aneurysm (33/176 alleles) or those with multiple aneurysms (6/28 alleles). Conclusion:Six base insertion polymorphism in Endoglin gene was not found to be a risk factor for intracranial saccular aneurysms in the South Indian population. Ethnic-related differences were observed. This is the first report on any genetic mutation in intracranial aneurysms in Indian population. Keywords: Association, endoglin , intracranial aneurysm, south indian, subarachnoid hemorrhage Introduction Intracranial aneurysm (IA [MIM 105800]) is a fairly common condition that is often asymptomatic until the time of rupture. Rupture of IA is the foremost cause for spontaneous subarachnoid hemorrhage (SAH), associated with high rates of morbidity and mortality. Incidence of IA in India varies from 0.75-10.3%.[1],[2] Cerebral arteries are particularly vulnerable to aneurysm formation since they lack an external elastic lamina. These vessels shed most of their external supporting layers as they enter the skull and are considerably thinner and more fragile than vessels elsewhere in the body. The hemodynamic stress like high blood pressure and pulsations can lead to the formation of saccular aneurysms carrying a risk of rupture that varies with their location, size and wall thickness.[3] Structural weakness of the arterial vessel wall may be due to genetic variants of genes responsible for the proper maintenance of vascular wall integrity.[4] Risk factors, such as smoking and hypertension seem to predict fatal SAH, independent of aneurysm size or patient age or sex.[5] Endoglin gene (ENG [MIM 131195]) codes for a homodimeric integral membrane glycoprotein, predominantly expressed on the vascular endothelium.[6] The ENG gene is located on Chromosome 9q33-q34.1 and modulates angiogenesis and vascular development. Association of a six-base insertion (6bINS) in intron 7 of Endoglin gene remains inconclusive due to ethnic differences.[7],[8],[9],[10],[11] In the present study we sought to investigate the association of the 6bINS (5′-TCCCCC-3′) polymorphism starting at 22 bp distal from the 3′ end of the exon 7 in the ENG gene as a risk factor for sporadic IA in an Indian population. Materials and Methods The study population consisted of 102 unrelated patients who had been consecutively admitted to a tertiary care referral hospital in South India during the period from May 2003 through January 2005. The diagnosis of aneurysm was done by cranial computed tomography (CT). The location of the aneurysm and its single or multiple nature was established by digital subtraction angiography (DSA). Patients with dissecting and fusiform aneurysms, arteriovenous malformations and hematological disorders were not included in the study. Clinical characteristics of patients with IA are summarized in [Table - 1]. The patient group consisted of 54 males and 48 females; mean ± SD age, 50.4 ± 11.4 years. The control group consisted of healthy, age and ethnically matched volunteers who did not possess any symptom of neurological disorders. Patients and controls belonged to the southern states of Kerala and Tamil Nadu with linguistic affiliation to Dravidian languages. The study was approved by the Institutional Ethical Committee for Biomedical Subjects, as per the ICMR guidelines. PCR amplification Three milliliters of peripheral venous blood from each patient was used for isolation of genomic DNA using the standard organic extraction protocol. Intron 7 region of the Endoglin gene was amplified by polymerase chain reaction using following primers 5′-GAGGCCTGGCATAACCCT-3′ and 5′-GTGGCCACTGATCCAAGG-3′.[10] Genomic DNA (100 ng) was amplified using 10 pmol of each primer, 250 mM deoxynucleotide triphosphate (Amersham), 1.9 mM MgCl 2, 1X PCR buffer and 0.5 U AmpliTaq Gold polymerase (ABI). Amplifying conditions were as follows: initial denaturation at 94°C for four minutes, followed by 35 cycles of denaturation at 94°C for 30 seconds, annealing at 60°C for one minute and extension at 72°C for one minute by using a thermal cycler (BioRad). Heteroduplex analysis 10 ml of each PCR product was denatured at 95°C for five minutes and slowly cooled (1°C/ minute) to 37°C and were kept on ice until loading. The renatured samples were loaded along with 2ml of loading buffer (0.25% bromophenol blue, 0.25% xylene cyanol FF and 30% glycerol) in 12% nondenaturing polyacrylamide gel containing 1 M urea and electrophoresed at room temperature in 1 X TBE buffer at 120V for three hours and subsequently stained with ethidium bromide (0.5 mg/ml). The presence of the insertion in either the heterozygous or homozygous insertion genotype was revealed by the formation of heteroduplexes, which was absent in the homozygous wild type sequence. Cloning of the PCR product To confirm the nature of the insertion in the heterozygous state, the PCR product was purified with GFX Column (Amersham), cloned into a pGEMTvector (Promega) according the manufacturer′s protocol and transformed into JM109 competent cells. Transformed colonies were selected by blue-white screening on LB agar plates containing Ampicillin (100 mg/ml). Colony PCR was done for the positive clones and the products were run on 1.2% agarose gel to confirm presence of 290 bp insert and analyzed by HA followed by DNA sequencing. This confirmed the presence of both wild type and insertion alleles, in an individual having heterozygous genotype. DNA sequencing The genotypes of all the cases and controls were further ascertained by sequencing. The PCR products were electrophoresed on a 1.2% agarose gel and bands were cut out and eluted for sequencing. Six micro liters of the eluted PCR product was used for sequencing using 0.64 mmol/L of the forward primer, used for genotyping. Cycling reactions conditions are as follows: for 25 cycles, ramp (1°C/ second) to 96°C for 10 seconds and ramp (1°C/ second) to 60°C for four minutes. Sequencing reactions were done using BigDye Terminator Cycle Sequencing v3.1 Kit and analyzed using ABI PRISM 310 Genetic Analyzer (Applied Biosystems). The homozygous wild type, heterozygous and homozygous insertion allele sequences were determined by sequencing [Figure - 1]. Statistical analysis Data was classified according to the genotypes of the Endoglin gene and the allele frequencies were calculated. Expected and observed frequencies of genotypes as well as Hardy-Weinberg proportions of allele distribution were assessed by Chi-square analysis. Comparison of genotypes between cases and controls were done using Armitage′s trend test. Odds ratios with 95% confidence intervals were calculated on 2 x 2 contingency tables using GraphPad Prism Ver 4. Probability value £ 0.05 was considered statistically significant. The power of the present study was calculated using the allele frequencies reported by Takenaka et al[6] for the 6bINS polymorphism, at a 5% test level (alpha=0.05, two-tailed). Results We investigated the INS polymorphism in the ENG gene in 102 patients with intracranial saccular aneurysms (48 women and 54 men, aged 51.4 (SD 11.4) years). The control group was matched for age (mean: 49.9 (SD 12.8) years) and sex ratio (59 women and 59 men). Other features that coexisted with intracranial saccular aneurysm patients were hypertension in 38 patients (37.3%), diabetes mellitus in seven (6.9%), alcohol consumption in 20 (19.6%) and active smokers in 36 (35.3%). Nine patients manifested multiple aneurysms and as a result 116 aneurysms were observed in 102 patients. These aneurysms were localized as follows: anterior cerebral artery complex; 48 (41.4%), internal carotid artery complex; 24 (20.7%), middle cerebral artery complex; 21 (18.1%) and vertebrobasilar artery complex; 23 (19.8%). The insertion allele polymorphism was found in 39 (19.1%) of 204 alleles in the patient group and in 42 (17.8%) of 236 alleles in the control group. Allele frequencies did not differ significantly in the Indian IA patients versus controls (χ 2= 0.13, df=1, P =0.72). Genotype frequencies did not differ significantly between the sexes ( P =0.35). There was no significant difference in the allele and genotype frequencies between cases and controls [Table - 2]. The -/-, +/- and +/+ genotype frequencies in the control subjects were 67, 30.5 and 2.5% respectively and were very similar to those expected under Hardy-Weinberg equilibrium (67.6, 29.2 and 3.2%, respectively, χ 2=0.216, P =0.89). There was also no relation between patients who harbored single aneurysm and those who harbored multiple aneurysms for the INS allele; 33/176 (18.7%) in the former and 6/28 (21.4%) in the latter ( P =0.80). The odds ratio of IA associated with the insertion allele was 1.09 (95% CI, 0.674 to 1.769) and with the homozygous insertion genotype, 0.89 (95% CI, 0.66 to 2.08). We do observe ethnic differences in the prevalence of 6bINS allele frequencies in world populations [Table - 3]. Discussion This study is the first report on the role of the Endoglin gene polymorphism in Indian population. The present analysis demonstrated a power of 80% at a 5% chance of observing an association between the 6bINS and intracranial aneurysms. Multi-factorial diseases like IA are likely to involve a number of different contributing genes, which may harbor ethnic-related differences of genetic polymorphisms. In one of the earliest report the 6bINS polymorphism in the endoglin gene was reported to be associated with IA in Japanese population, where the INS allele polymorphism was 40.9% in the patient group and 27.6% in the control group (χ 2=7.48, P =0.006).[7] However, another study in the Japanese population failed to confirm the association, with the INS allele frequency at 30.2% in the patient group and 31.9% in the control group. In addition, a multipoint linkage analysis using 20 micro satellite markers spanning Chromosome 9 in 104 Japanese sib pairs showed no evidence of linkage in the vicinity of the Endoglin gene.[9] In a study conducted in the German population, an additional control group of healthy, unrelated Japanese volunteers were also analyzed and the INS allele frequency was found to be 33.3%, i.e., 10 out of 30 alleles.[8] From all the Japanese control groups analyzed independently in three different studies, it was seen that the INS allele frequency in the Japanese ranged from 27.6 to 33.3%. This was nearly twice as high as those reported in the Germans (14.4%), North American (19.8%) and Polish (16.0%) control groups. Although the frequency of the INS allele found in our study was similar to that reported in the Caucasian population, it was significantly lower when compared to the Japanese population ( P =0.01). This suggests that cross-cultural comparisons should be avoided for genetic association studies, as ethnic-related differences in the Endoglin gene exists, which may lead to wrong interpretation. Many factors influence contradictory findings across studies, which include measurement error with respect to genotyping and the behavioral phenotype, measurement error with respect to the phenotype, differences in designs and confounding variables such as population stratification. The threat of population stratification in the case-control design is often the scapegoat when an effect demonstrated in one study is not found in another. Conclusion Our results indicate ethnic differences in 6bINS allele frequencies when compared to other world populations but does not support the hypothesis that the 6bINS allele is associated with the development of intracranial saccular aneurysms or with any symptomatic aggressiveness of IA in South Indian population. Acknowledgments This study was supported by a fellowship from the University Grants Commission (UGC), New Delhi, India. LKV and HVE contributed equally to the research work. References
Copyright 2006 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg06020t1.jpg] [hg06020t2.jpg] [hg06020f1.jpg] [hg06020t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}