 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
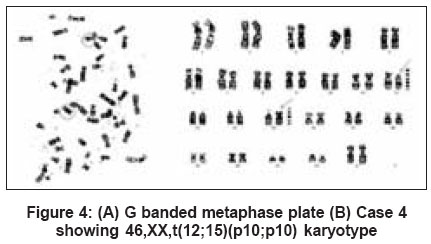
Indian Journal of Human Genetics, Vol. 12, No. 3, September-December, 2006, pp. 133-139 Brief Report Chromosome 12;15 rearrangements in patients with recurrent miscarriage Nair SB, Mukundan G, Paul BM, Ramachandran L, Gopinathan KK, Joseph Sajayan CIMAR Genetics, Department of Fetomaternal Medicine, Edappal Hospitals, Kerala Code Number: hg06025 Abstract Background: An abnormal karyotype in either partner, especially featuring a translocation and/or inversion is considered to be a cause of recurrent miscarriages. It is generally assumed that recurrent miscarriage might be due to recurrent chromosomal abnormalities in the fetus due to a balanced aberration in one of the parents being inherited by the offspring in an unbalanced form. Keywords: Chromosomal rearrangements, cytogenetics, GTG banding, pregnancy loss, reciprocal translocation, recurrent miscarriage, robertsonian translocation Introduction Pregnancy loss is defined as the unexpected and unplanned spontaneous loss of pregnancy before the fetus becomes capable of extrauterine survival. Numerous different factors have been suggested to contribute to this. These factors can be grouped under specific classes, such as chromosomal, genetic, maternal (anatomic features and maternal diseases), endocrinologic, immunologic, disorders of coagulation and exogenous.[1] The single most common reason for pregnancy loss is the presence of a chromosome abnormality in the fetus, particularly if the loss occurs early in the pregnancy. About 60% of recurrent miscarriages (defined as the loss of three or more consecutive pregnancies before 20 weeks of pregnancy) might be caused by chromosomal aberrations in the embryo.[2] In recurrent miscarriage, it is common clinical practice to karyotype both parents for chromosome aberrations as officially recommended by both the American[3] and Royal[4] College of Obstetricians and Gynecologists. About 5.5% of couples experiencing three or more losses have one partner who carries a chromosomal rearrangement, in comparison to less than 0.55% of the general population.[5] These rearrangements are detected twice as often in the female partner with a history of pregnancy loss.[6] The most commonly observed rearrangements are either reciprocal or Robertsonian translocations.[1] A translocation results from the exchange of chromosome segments between nonhomologous chromosomes. If the transfer of genetic information between two chromosomes appears to be complete and is not associated with a loss of material, the translocation is reciprocal and balanced. Robertsonian translocations are associated with a loss of genetic material, but generally not associated with phenotypic abnormalities and originate through translocations of the acrocentric chromosomes.[7] Balanced translocations occur in approximately one in 500 individuals.[8] The majority of balanced translocation carriers do not have any associated clinical problems except decreased fertility and the risk of abnormalities to their offspring as a result of malsegregation due to the translocation.[7] Fryns and Van Buggenhout[9] reported that of the chromosomal abnormalities observed in couples with two or more pregnancy losses, two-thirds were balanced autosomal translocations with the incidence of such translocations in this group being 30 times higher than in the general population. However, only one-third of these losses result from an unbalanced fetal karyotype related to the rearrangement in the parent, suggesting that translocation carriers may be at increased risk for other types of aneuploidy.[10] Prospective studies of couples identified as balanced translocation carriers indicate that as many as 80% of their pregnancies end in abortions (giving birth to an embryo or fetus prior to the stage of viability at about 20 weeks of gestation), while 16% lead to the birth of a healthy newborn.[1] This reduction in the frequency of chromosomal abnormality between conception and delivery is due to the selective loss of fetus with chromosomal abnormality during gestation. Carriers of reciprocal translocations are thought to have higher frequencies of spontaneous abortions, (abortion that occurs from natural causes) but the clinical miscarriage rates and subsequent pregnancy outcome for different abnormalities have not been reported in detail.[11] History of an abnormal offspring is about fourfold likely if it is the mother who carries the rearrangement. Translocations can be inherited (familial) or de novo (newly occurring).[7] A total of 467 couples with history of recurrent miscarriage were presented to our clinic from peripheral centers between Jan 2000-Jun 2006. Investigations were carried out to rule out nongenetic factors such as placental abruption, preclampsia etc as the causative factor for multiple abortion. After that they were enrolled for genetic work-up. Both partners of each couple were karyotyped and out of that we found 30 cases with translocations. Here we report four cases of rare balanced autosomal translocation involving Chromosome 12 and Chromosome 15. Materials and Methods The four couples who reported here were thoroughly examined to rule out other nongenetic causes of pregnancy losses and detailed clinical and family histories were recorded in a predesigned proforma. The predesigned proforma included details of couples like obstetric history, time and number of abortions, parity, living children, family history of recurrent abortions, consanguinity, caste, religion and ethnicity etc. These patients were referred from peripheral centers to our Center for Infertility Management and Assisted Reproduction (CIMAR), Edappal Hospitals Pvt. Ltd, Edappal, Kerala, India for the diagnosis and management of repeated fetal loss. A written informed consent was obtained from all patients. Case 1 A 34-year-old phenotypically normal female presented with three missed abortions in the first trimester. Her partner was found to be phenotypically and clinically normal. All the other clinical parameters of both the partners were within the normal range. Presently they have a chromosomally normal male and a female child. No relevant family history and consanguinity were observed. Case 2 A 22-year-old phenotypically normal female with three missed abortions in the first trimester was referred to our center. Her mother also had a history of five missed abortions - four in the first trimester and one in the second trimester but she was unavailable for karyotyping. Her partner was a 31-year-old phenotypically normal male. His sperm count was normal. All the other clinical parameters of both the partners were within the normal range. No consanguinity was seen. Case 3 A 38-year-old phenotypically normal female reported with four missed abortions in the first trimester. After the 4th abortion she had post-abortal endometritis. Her partner was 48 years old and was phenotypically normal. All the other clinical parameters of both the partners were within the normal range. No relevant family history and no consanguinity were observed. Case 4 A 37-year-old phenotypically normal female with three missed abortions and two neonatal deaths was referred to our center for prenatal diagnosis at 17-18 weeks of gestational age. Her partner was found to be phenotypically and clinically normal. They already had a normal female child. No relevant family history and no consanguinity were observed. Prenatal diagnosis of the fetus was done by long-term culture using amniotic fluid. Karyotyping revealed a fetus carrying a translocation. The couple was given genetic counseling. Peripheral blood of the parents were drawn and lymphocyte cultures were put up for karyotyping to trace the origin of the translocation. Peripheral blood lymphocyte culture Peripheral blood lymphocyte culture was carried out according to the standard protocol[12] with slight modifications. Five ml of blood was collected by vein puncture in a sterile heparinised syringe under aseptic conditions and was gently mixed to avoid clotting. Peripheral whole blood cultures were set up by inoculating 0.5 ml blood in 5 ml of culture medium (RPMI 1640; Sigma, USA) at pH 7.4, supplemented with 10% of fetal bovine serum (Gibco BRL). To initiate the cultures 0.1 ml of phytohaemagglutinin (Lectin; Sigma, USA) was added. The cultures were incubated at 37 o C in CO 2 incubator for 72h. At the 69th hour, 150 μl of colchicine (Sigma, USA) from a stock solution of 10 μg/ml was added to the cultures to arrest the cell division at metaphase stage. Harvesting The cultures were harvested on the third day after two hours of colchicine treatment. These were then centrifuged at 1000rpm for 10 minutes. The supernatant was discarded. The cells were resuspended in 5 ml of prewarmed 0.56% hypotonic solution (KCl, Sigma, USA) and incubated in a waterbath maintained at 37°C for 4 ½ minutes. They were centrifuged again at 1000 rpm for 10 minutes. The supernatant was discarded and the cells were fixed in chilled acetomethanol (1:3) fixative. Two to three fixative washes were given until a clear cell suspension was obtained. Slide preparation The slides were previously cleaned by keeping in chromic acid overnight, followed by washing in running tap water. Slides thus cleaned were kept in distilled water at 4°C. Three to four drops of cell suspension were dropped evenly on a chilled wet slide using a Pasteur pipette and dried on a slide warmer at 37 osub C. The slides were labeled and stored at room temperature. GTG banding (G bands by trypsin using giemsa) The technique of Sun et al[13] was followed with slight modifications, as the routine banding method. Prepared slides were treated with 0.5% Trypsin solution (Sigma, USA) prepared in phosphate buffered saline (PBS) for about 5-20 seconds. The slides were rinsed thoroughly in two changes of PBS and stained in 10% Giemsa (Sigma, USA) solution for 10 minutes. The slides were again rinsed in distilled water, allowed to dry and then observed under the microscope. In all the cases 20 well-spread G-banded metaphases were karyotyped using Olympus BX60 microscope and Cytovision software (Applied Imaging). Result One of the partners in each case represented a balanced chromosomal rearrangement involving Chromosomes 12 and 15. Case 1 The female partner of case 1 though phenotypically normal had a balanced translocation; 46,XX,t (12;15) (q15;q25) [Figure - 1]. Karyotype of the male partner however was normal 46,XY. Case 2 The karyotype of the female partner of the second case revealed a balanced translocation involving Chromosomes 12 and 15, 46,XX,t (12;15) (q14;q26) [Figure - 2], though she had a normal phenotype. The male partner had a normal karyotype of 46,XY. Case 3 The female partner of this case was normal phenotypically as well as genotypically (46,XX). The male partner was phenotypically normal. However, karyotype analysis revealed a balanced translocation, 46,XY,t- (12;15)(q14;q25) [Figure - 3]. Case 4 Prenatal diagnosis in this case showed that the fetus had a translocation involving Chromosomes 12 and 15, the karyotype being 46,XY,t (12;15) (p10;q10). On further evaluation, the female partner of the couple was also found to have the same translocation, 46,XX,t(12;15) (p10;q10) [Figure - 4] while, the male partner had a normal karyotype of 46,XY. Since the mother had the same translocation as that of the fetus and she was phenotypically normal, it was inferred that the translocation was a balanced reciprocal translocation. The couple was offered genetic counseling and advised to continue the pregnancy. Discussion We present here four cases of balanced translocation involving Chromosomes 12 and 15 in patients referred with recurrent miscarriage. In three cases the rearrangement was found in the female partners while in one of the case the male partner carried the translocation. The karyotypes were found to be as follows: Case 1 - 46,XX,t (12;15) (q15;q25) in the female partner; Case 2 - 46,XX,t (12;15) (q14;q26) in the female partner; Case 3 - 46,XY,t (12;15) (q14;q25) in the male partner; Case 4 - 46,XX,t (12;15) (p10;q10) in the female partner. In our findings, none of the four cases showed any numerical aberrations. Cases 1, 2 and 3 had translocation involving the q arms of Chromosome 12 and Chromosome 15 whereas in case 4 the p arms of the same chromosomes were found to be translocated. With the limitations of GTG banding it was observed that a segment of Chromosome 12 has been translocated to chromosome 15. Since the carriers of the translocation were phenotypically normal, the translocation is assumed to be balanced and reciprocal. FISH technique would be useful for further evaluation. According to some of the studies, up to 60% of sporadic miscarriages[14],[15] and between 29-60% of recurrent miscarriages might be caused by chromosomal aberrations in the embryo.[16],[17],[18] It is generally assumed that recurrent miscarriage may be due to recurrent chromosomal anomalies in the fetus as a balanced aberration in one of the parents could be transmitted to the offspring in an unbalanced from. The parental chromosomal aberration might be either a structural anomaly, such as reciprocal or Robertsonian translocation or mosaicism for numerical aberrations.[2] Carriers of balanced translocations are subjected to an increased risk of abnormal chromosomal segregation during meiosis. The consequences include infertility, multiple pregnancy losses and live born abnormal offspring with multiple congenital malformations as a result of chromosomal imbalance. A chromosome with a reciprocal translocation forms a quadrivalent with matching homologous segments at meiosis I. This is followed by alternate segregation, adjacent-1, adjacent-2, 3:1 segregation or 4:0 segregation. Unbalanced gametes formed from reciprocal translocations detected by recurrent miscarriage can be speculated to be weeded out by natural selection, because the imbalance is too severe for gametes to survive. The majority of spontaneous abortions occur in pregnancies with incomplete fetal development. However, abnormal development does not always end in spontaneous abortions as is evident from the 3-4% population incidence of sporadic congenital anomalies.[1] Pregnancy outcome is also related to the size and genetic composition of the rearranged portions of the chromosomes. This gives the possible explanation of multiple pregnancy loss in patients with a balanced autosomal translocation, which is in accordance with our data. There are many causes of recurrent miscarriage including antiphospholipid antibodies, uterine anomalies and immunologic abnormalities. One major genetic reason for recurrent miscarriage is found to be a balanced translocation in either of the parents. Ogasawara et al[11] reported that almost all embryos with unbalanced gametes might miscarry in cases with a history of recurrent miscarriage whereas those whose parental translocation is detected because of a history of live births with congenital abnormalities might be born with unbalanced gametes and congenital abnormalities. Any discrepancy between miscarriage and congenital anomalies caused by unbalanced gametes might depend on the chromosome number and the positions of breakpoints. Several studies have been carried out to determine the prevalence of chromosomal aberrations among couples with repeated pregnancy loss.[19] In a study of 1284 patients with recurrent miscarriages, Ogasawara et al[11] reported that 7.79% had an abnormal karyotype in at least one partner and 1.8% had a balanced reciprocal translocation. According to Shafeghati et al more than 50% of spontaneous first trimester abortion specimens that undergo karyotyping were found to have a chromosomal abnormality. In 2.78-3.4% cases of couples with two or more pregnancy losses, Shafeghati et al[20] found that one of the couples was a balanced translocation carrier. Their data revealed that the most common type of abnormality in these kinds of cases is a translocation. A recent study[21] of 742 couples from Delhi, India showed 2% chromosomal abnormalities in subjects with recurrent spontaneous abortions, of which structural abnormalities formed the largest group. Reciprocal translocations were seen in 68% and the female to male ratio was 2.1:1. In our study, one couple had a history of two neonatal deaths where the infants expired due to multiple congenital abnormalities and they were not available for cytogenetic investigation. No other couple had live births with an unbalanced karyotype. The risk of having a handicapped child with an unbalanced karyotype depends on the type of translocation and on the sex of the transmitting parent.[22],[23] Al Hussain et al[19] in their study on couples with recurrent abortions in Saudi Arabia reported that the carriers of the translocation were predominantly females. This may be due to the fact that chromosomal abnormalities that are compatible with fertility in females may be associated with sterility in males. In another study by Testart et al ,[24] the frequency of translocations and inversions were found to be greater in men than in women in couples who underwent intracytoplasmic sperm injection (ICSI) treatment. Since a high frequency of structural chromosomal abnormalities is reported in sperm with poor motility, a lower fertility and therefore lower miscarriage rate with male reciprocal translocation carriers can be speculated.[25] In our present study, 30 cases of translocations were found, of which we reported here only couples with translocation 12;15. Three out of the four carriers in this study were females. This is in agreement with the studies of Al Hussain et al ,[19] even though the number of cases included in the study was less. Carp et al[2] studied 916 patients with three or more consecutive miscarriages before 20 weeks′ gestation. Their study showed that the prevalence of chromosomal aberrations was independent of the number of previous abortions. The type of aberration had no appreciable effect on the subsequent live birth rate, whether the aberration was a translocation, inversion or numeric mosaicism. Additionally there was no effect if the aberration was maternally or paternally derived. Analysis of live birth rate according to the number of previous miscarriages showed that the incidence of live births decreased with the number of previous miscarriages, but there was no significant difference in the birth rates for any particular number of abortions. The implication of the present study is that, it is important to detect these cases as early as possible to arrange for adequate genetic counseling and to allow parents to make an informed reproductive decision regarding subsequent pregnancies. The only form of therapy that can overcome the presence of chromosomal aberrations in the embryo is preimplantation genetic diagnosis (PGD). This technique has been reported to result in an approximately 25-30% pregnancy rate per transfer.[26],[27] Our search for literature on chromosome 12;15 translocation in patients with repeated pregnancy losses yielded no result. The rarity of this translocation and the detection of four such cases in the present study indicate that some nongenetic factors might have a role to play in predisposing the individuals to such chromosomal aberrations. To the best of our knowledge these four cases are the first to be reported in which a segment of the Chromosome 12 gets translocated to Chromosome 15 in patients with recurrent miscarriage. However, FISH technique would be useful in determining the exact regions of translocation. Genetic counseling was offered to all the four couples and the risk factor for future pregnancies was described in detail. Safety measures like prenatal diagnosis and PGD were discussed. References
Copyright 2006 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg06025f1.jpg] [hg06025f4.jpg] [hg06025f2.jpg] [hg06025f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}