 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
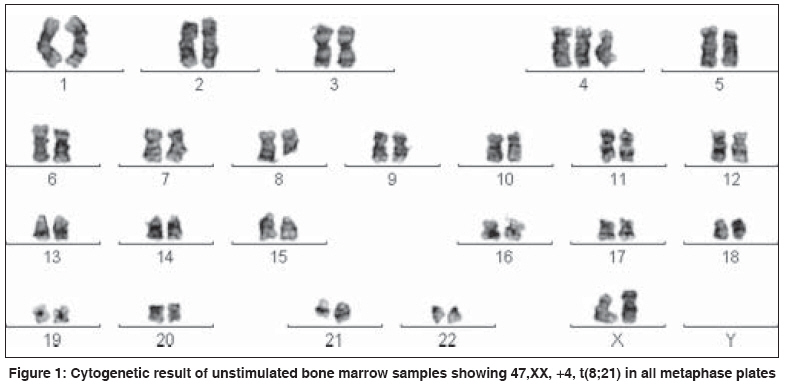
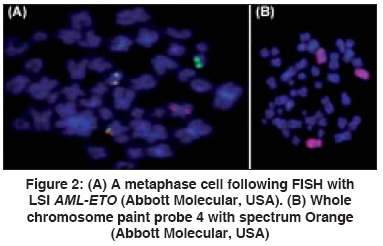
Indian Journal of Human Genetics, Vol. 14, No. 1, January-April, 2008, pp. 20-22 Case Report A case of acute myeloid leukemia-M2 with trisomy 4 in addition to t(8;21) Trivedi PJ, Patel PS, Brahmbhatt MM, Patel BP, Gajjar SB, Iyer RR, Parikh EH, Shukla SN, Shah PM, Bakshi SR Cell Biology Division, The Gujarat Cancer and Research Institute, NCH Campus, Asarwa, Ahmedabad - 380 016 Code Number: hg08005 Abstract t(8;21)(q22;q22) is the most frequently observed karyotypic abnormality associated with acute myeloid leukemia (AML), specifically in FAB-M2. Short-term unstimulated bone marrow (BM) and peripheral blood lymphocyte culture showed 47,XX, +4,t(8;21) in all metaphase plates; and interphase and metaphase results of AML-ETO fusion was positive and trisomy of 4 was confirmed with WCP probes. Trisomy 4 in AML with t(8;21) is a rare numerical abnormality. Here we present such case of patient which may constitute a distinctive subtype.Keywords: Acute myeloid leukemia, cytogenetics, fluorescence in situ hybridization Introduction t(8;21)(q22;q22) is the most frequently observed karyotypic abnormality associated with acute myeloid leukemia (AML), specifically in FAB M2. Trisomy 4 as the sole anomaly is a rare chromosomal abnormality associated with a specific subtype of primary acute non lymphocytic leukemia (ANLL) and secondary (treatment-related) ANLL with myelomonocytic morphology; it has been found with the same frequencies in the M1, M2, and M4 FAB phenotypes. [1],[2] A retrospective analysis on the clinical and laboratory data of 21 cases of acute leukemia (AL) with trisomy 4 was performed by Pan et al. and showed that AL with trisomy 4 have unique clinical and laboratory features and a poor prognosis. M2 was the most frequent subtype in this series (9 out of 21 cases). [3] Association of +4 with double minute chromosomes has been described in 10 cases; 5 with AML-M2, 2 with AML-M4, 1 with refractory anemia with excess of blasts in transformation (RAEB-T), one with chronic myelomonocytic leukemia (CMMoL), and one with unclassified preleukemia. The coincidence of +4 with t(8;21) or its variant t(6;21;8) has been observed in at least two cases of ANLL (M1 and M2), is therefore recurrent. Apparently, trisomy 4 has no prognostic sifgnificance in ANLL; with the exception of the cases bearing c-kit mutations that are associated with a rapid disease progression. Trisomy 4 has been described in two cases of T-cell acute lymphoblastic leukemia as the sole chromosomal anomaly. Combined trisomies of chromosomes 4 and 10 are reported in children with B-progenitor cell acute lymphocytic leukemia and has shown a favorable prognostic association. Patients with chromosomes 4 or 10 trisomies as a sole anomaly have an extremely favorable 44-year event free survival after antimetabolite-based chemotherapy. [4]Case Report A 60-year-old female with complaints of general weakness was registered at Gujarat Cancer and Research Institute in May 2007. Peripheral blood report was hemoglobin concentration 7.8 g/dL, White Blood Cell count 0.03 x 10 9 /L, polymorphs 7%, lymphocytes 14%, myelocytes 4%, blast cells 75%, and Platelet count 0.0046 x 10 9 /L. Peripheral blood smear showed presence of blasts with Auer rods. Bone marrow report revealed hypercellular marrow with marked depletion of all the normal marrow precursor cells. Few blasts showed presence of Auer rods in cytoplasm, Sudan Black-B was positive, and periodic acid Schiff (PAS) was negative, M:E ratio was altered, and megakaryocytes were not seen, lymphocytes 8%, eosinophills 1%, polymorphs 3%, band cells 2%, metamyelocytes 1%, myelocyte 8%, promyelocytes 3%, and blast cells 72%. Final diagnosis based on morphological and cytochemistry findings was AML with M2 subtype as per French-American-British classification. Constitutional nature of trisomy 4 could not be ruled out. After 1 month of sample received, the patient was lost to follow up. Chromosome preparation Fluorescence in situ hybridization (FISH) assay Chromosome analysis FISH analysis Discussion Trisomy 4 is a rare nonrandom cytogenetic abnormality found in association with AML. The Mitelman database for chromosomal aberrations in cancer queried for trisomy 4 with t(8;21) in AML showed only two cases. [6] Gains or losses of chromosomes are frequent findings in AML, more common being monosomy 7 and trisomy 8. Most of such changes are not restricted to any specific FAB types of AML, are often also associated with secondary AML and AML with pre-existing myelodysplasia, or during clonal progression of AML. Rarely gain of chromosome 4 or chromosomes 10 are reported as the sole abnormality in AML. Some morphologic subtypes of AML are associated with specific chromosomal abnormalities. Most of these abnormalities are chromosomal translocations which amplify or activate chimeric genes situated near the breakpoints of translocations. Trisomy 4 occurs in AML with frequency of < 1% and a strong association with the presence of double minutes has been described. Double minutes were not observed in our patient. CD56 expression in AML is reported in granulocytic sarcoma and multidrug resistance, and is known to confer poor prognosis in AML-M2 with t(8;21) and acute promyelocytic leukemia. It has been suggested that there might exist a dosage effect of certain genes resulting in growth advantage of malignant cells. In the case of AML with trisomy 4 and double minutes, V-myc myelocytomatosis viral oncogene homolog (avian) amplification is a common finding. Jennings et al, have also suggested that acquisition of trisomy 8 leading to MYC locus amplification might underline the molecular mechanisms for the clonal progression of chronic myeloid leukemia. A direct link between chromosomal gain, oncogenes amplification, and leukemogeneisis has yet to be established. [7],[8] Our patient was lost to follow up hence the CD56 status was unclear. Therefore, relation between CD56 expression and trisomy 4 needs further investigation. While development of AML with trisomy 4 secondary to chemo or radiotherapy has also been suggested, our patient had no history of long-term medication, radiotherapy, or any relevant occupational exposure. In conclusion, based on the morphological, cytochemistry, and clinical features the present case of AML-M2 is a rare case in terms of cytogenetic results. Even though trisomy 4 is likely to be a secondary event after t(8;21) translocation, the presence of this additional numberical aberration may define a distinctive subtype. Follow up of more such cases over a period of time is required to know the possible prognostic effect of this cytogenetic entity. [9] References
Copyright 2008 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg08005f1.jpg] [hg08005f2.jpg] |
| |||||||||

{kind=link}
{kind=link}