 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
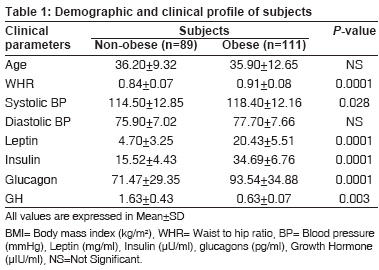
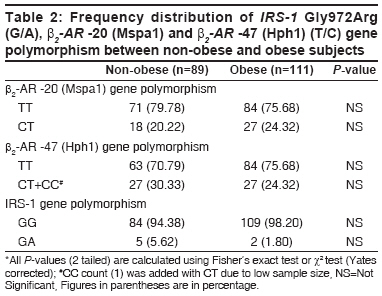
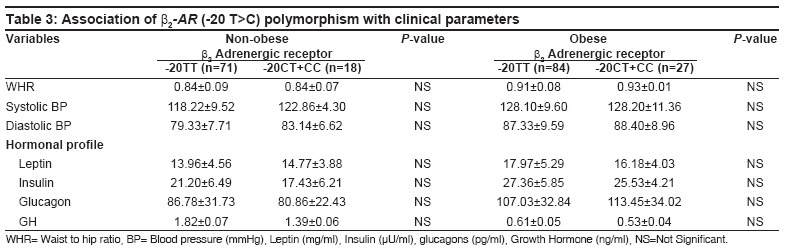
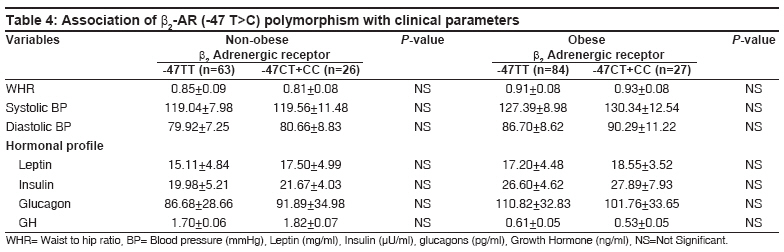
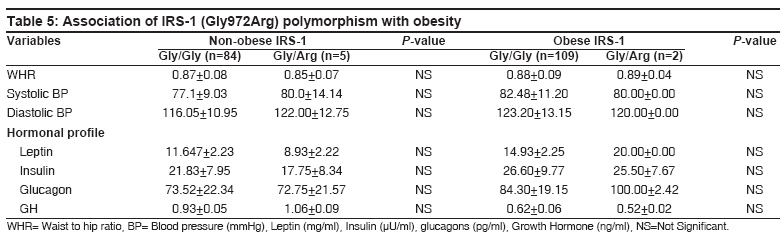
Indian Journal of Human Genetics, Vol. 14, No. 2, May-August, 2008, pp. 48-54 Original Article Association of β2-adrenergic receptor and insulin receptor substrate-1 polymorphisms with obesity in a Northern Indian population Srivastava Neena, Achyut BR, Prakash Jai, Agarwal CG, Pant DC, Mittal Balraj Department of Genetics, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow Code Number: hg08012 Abstract Background: Imbalance in hormonal levels, regulated by host genetic factors, are known to be a major cause of obesity. Therefore, we aimed to evaluate association of genetic polymorphisms of β2 -adrenergic receptor (β2 -AR) and insulin receptor substrate-1 (IRS-1) with hormonal levels in northern Indian obese.Methods: A total of 111 obese and 89 age matched non-obese subjects were studied after taking detailed clinical profile. Hormonal assays in serum/plasma for different hormones were done using IRMA and RIA kits. Genetic analysis of β2 -AR (-47 and -20, T to C) and IRS-1 (Arg972Gly) was done using PCR-RFLP. Statistical Analysis: Statistical analysis was performed by SPSS (version 11.5) software. All continuous variables were expressed as mean ± SD and tested by ANOVA test. Comparisons of categorical variables were assessed using X2 tests or Fisher's exact test. P-value <0.05 was considered as significant. Results: Analysis showed that obese subjects had significantly higher value of blood pressure (systolic), WHR, leptin insulin and glucagon and lower value of GH. In β2 -AR (-47) T/C and IRS-1 Gly972Arg gene polymorphisms we did not found significant differences in genotype or allele frequencies. Moreover, none of the studied hormonal or metabolic parameters showed any association with the gene polymorphisms. Conclusions: Study reveals no significant association of β2 -AR (-47 and -20, T to C) and IRS-1 Gly 972 Arg polymorphisms with obesity in northern Indians. Keywords: Association, genetic polymorphism, hormones, obesity Introduction Obesity has become a global pandemic and long standing obesity is often among one of the risk factors for metabolic syndrome. Though studies have been performed on causation of obesity but none of the researchers showed association of such a large range of factors together. Obesity being a multifactorial disorder, in the present study we tried to associate various demographic and hormonal factors with obesity. Further, the study was extended to confirm the existence of genetic factors with obesity. In this study, we want to explore the relationship between all these demographic, hormonal, and genetic factors in obese north Indians. Obesity is considered to be a complex trait, influenced by both environmental and host factors. Host factors include different metabolic factors and hormones that play a vital role in regulation of obesity. Female gender and older age are known to be a risk factor for obesity. [1],[2] Insulin, leptin, growth hormone, thyroid hormones, and glucagon have a great influence in causation of obesity. Insulin resistance and its pathophysiologic sequalae include hypertension, dyslipidemia, atherosclerosis (metabolic syndrome or syndrome X). [3] Hyperinsulinemia contributes to the characteristic alterations in plasma lipid profile. Studies have also highlighted the importance of abdominal subcutaneous fat as an independent marker of insulin resistance. [4],[5],[6] Leptin is a hormone released from the adipocytes which influences energy balance, exerts long acting effects to reduce adiposity by decreasing appetite and increasing thermogenesis. [2] A glucagon level regulates orexigenic-signal terminating meals after feeding. [7] In recent study, a positive association between higher fasting plasma glucagon like peptide and fat oxidation was observed thus reducing obesity. [8] Growth hormone secretion is impaired with any secretory defect of pituitary which is proportional to degree of obesity. There is conflicting information on interaction of growth hormone and its relation to cardiovascular risk and obesity. [9] Hypertension is being observed in obese subjects with high leptin levels. [10] Recent studies have shown increased expression and activation of the circulating vasoconstrictor enzymes in adipose tissue, elevating the blood pressure in obese individuals. [11] Thyroid hormones play an important role in regulating energy homeostasis by stimulating expression of adrenergic receptor by enhancing responsiveness of catecholamines and thus regulating obesity. [12] Apart from these factors, role of genetic polymorphisms has also been known to affect obesity phenotype. Kentaro et al. [13] were the first to identify two promoter polymorphisms (T to C) at -47 and -20 in 5′ leader cistron of β2 -AR gene and observed the high frequency of variant allele (-47 C) in obese as compared with non-obese subjects. After this report, known to our best, no study has been published so far showing the association of these promoter polymorphisms with obesity or other conditions. IRS-1, principal substrate for insulin and insulin like growth factor (IGF-1) receptors is involved in glucose clearance [14],[15] and is an attractive candidate gene to harbor genetic variation that might influence insulin resistance and obesity. Glycine to arginine amino acid substitution at 972 codon of its gene product leads to reduced activity. Although, several reports on obesity has been published but none of them studied such a wide range of factors together which are involved in causation of obesity. In the present study, we aimed to find out the association of demographic, hormonal and genetic factors like β2 -AR (-47 and -20 T/C) and IRS-1 Gly972Arg gene polymorphisms with obesity in north Indian population. Materials and Methods Subjects Sample collection Hormonal assays Genotyping for β2-AR (-20 and -47 C/T) Polymorphism Genotyping for IRS-1 Gly 972 Arg polymorphism Gels were stained with ethidium bromide and visualized under ultraviolet light. All PCR reactions were performed in a Thermal Cycler (MJ Research Inc, Waltham MA). Gel documentation was done by Alphaimager TM 1220, Alpha Innotech Corporation, USA. Statistical analysis Results The demographic and clinical profiles are shown in [Table - 1]. A total of 200 individuals (89 non-obese and 111 obese) with BMI (25.69±5.27 kg/m 2 ) waist to hip ratio (WHR) (0.87±0.08) and mean age 31.38±11.70 years were included in the present study. Association of BMI with demographic and hormonal profile Frequency distribution of IRS-1 Gly972Arg (G/A), β2 -AR -20 (MspA1) and β2-AR -47 (Hph1) (T/C) gene polymorphism in non-obese and obese The frequency of variant allele was very low. We found only one variant genotype (CC) so we include this in the heterozygous CT genotype. There was no significant difference in the frequencies of the TT genotype and CT genotype of β2 -AR -47 (Hph1) gene polymorphism between the non-obese and obese subjects. The frequency of GG, GA genotype of IRS-1 Gly972Arg gene polymorphism was also not significantly different in non-obese and obese subjects. Here also, no variant AA was found in non-obese and obese subjects. Association of IRS-1 Gly972Arg and β2 -AR -20 and -47 T/C polymorphisms with demographic and hormonal profile Discussion The combined effects of genes, environment, and lifestyle are responsible for development of obesity. In this study, BMI was taken as major criteria of obesity and correlation of BMI with different clinical and genetic parameter was seen like waist to hip ratio and hormonal levels (insulin, leptin, glucagon, and growth hormone). A statistically significant (P≤0.001) association of increased leptin levels (20.4±5.5 vs. 4.7±3.3) was observed in subjects with high BMI. The leptin level was significantly higher in obese females. These results are similar to the findings of Considine et al. [1] where leptin levels were 31.3±24.1 ng/ml in obese subjects and 7.5± 9.3 ng/ml in normal weight subjects (P< 0.001). Richard et al. [21] also found increased leptin levels in obese group (17.1± 4.8 vs. 5.8± 1.42 ng/ml, P=< 0.001) than normal subjects. Recent studies also revealed a correlation of BMI with increased leptin in obese women. [2] Subjects with higher BMI and WHR showed higher leptin levels in present study. This was in agreement (P< 0.001) with the finding of previous study conducted by Paul et al. [22] Richard et al.[21] reported negative correlation between waist to hip ratio and leptin levels, which was not statistically significant (P=0.99). GH level showed a significant fall with obesity in our study and these findings are in conformity with the observations of a recent study. [9] Savastano et al. [23] observed a negative correlation with age, BMI, waist circumference and fat mass which also favors this study. In this study, we investigated 2 genetic variants of the b2 AR gene and 1 genetic variant of IRS-1 gene as candidates to predispose obesity. Blood pressure as well as fat metabolism are regulated by the β2AR, so we tested the β2 AR polymorphisms for association with hypertension obesity. Genetic variance in the IRS-1 is thought to play a key role in the insulin resistance that characterizes type 2 diabetes. [24] So, we wanted to look for association of the polymorphisms in IRS-1 and β2 -AR genes. Our results showed that Gly to Arg variation in IRS-1 gene was observed in 7 (3.5%) subjects. Clausen et al. [25] found the increased insulin resistance with IRS-1 Gly 972 Arg polymorphism in heterozygous state in obese patients. Caucasian study performed in two cohorts found the increased insulin resistance in obese children. [26] Siqal et al. [27] reported that Gly to Arg polymorphism predisposes to NIDDM only in the presence of excess of body weight. Insulin promotes adipocyte triglyceride stores by a number of mechanisms stimulating tri-glyceride synthesis (lipogenesis). In adipocytes of obese human IRS-1 protein expression is down regulated, resulting in decreased IRS-1 associated phosphoinisitide 3 kinase (PI3K) activity which comes down stream in the insulin metabolism pathway and has antilipolytic action which is preserved in diabetic obese despite of low insulin levels resulting in maintenance or expansion of fat stores. Studies have shown that β2 -adrenergic receptor (ADRB2) controls energy balance and storage of fat. This receptor is down regulated in white adipose tissue in obesity. Its gene is known to be highly polymorphic. [28] Several polymorphisms in coding region and their haplotypes have been found to be associated with asthma, hypertension, diabetes and obesity. [29],[30],[31],[32] The most common polymorphism Arg16Gly was found to be associated with risk for obesity. [33] A study from western world showed that Arg16Gly polymorphism was associated with weight gain from childhood to young adulthood in males. [34] However, some contradictory observations have been seen in some of the studies. [35] Earlier study published from Japan [13] stated the importance of promoter polymorphisms in β2 -AR gene. Therefore, to find out if any association is present in Indian population, we performed the present study. However, this study also did not reveal any significant association of β2 -AR -20 and -47 T/C polymorphisms with obesity. In conclusion, the present study revealed significant association of demographic and hormonal factors with obesity in north Indians. No significant association of any obesity related factor could be established with β2 -AR promotor polymorphisms and IRS-1 Gly 972 Arg polymorphism. The limitations of this study is low sample size and the subjects consider as obese have BMI ≤25 rather then BMI ≤30. Moreover, frequencies of variant alleles in these polymorphisms were very low, and large sample size may be required to achieve definitive results of the association. Acknowledgment Authors acknowledge Indian Council of Medical Research, New Delhi and intramural grant from Chatrapati Shahuji Maharaj Medical University Uttar Pradesh, Lucknow, (UP) India, for the financial support to carryout this research work. References
Copyright 2008 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg08012t1.jpg] [hg08012t5.jpg] [hg08012t4.jpg] [hg08012t2.jpg] [hg08012t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}