 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
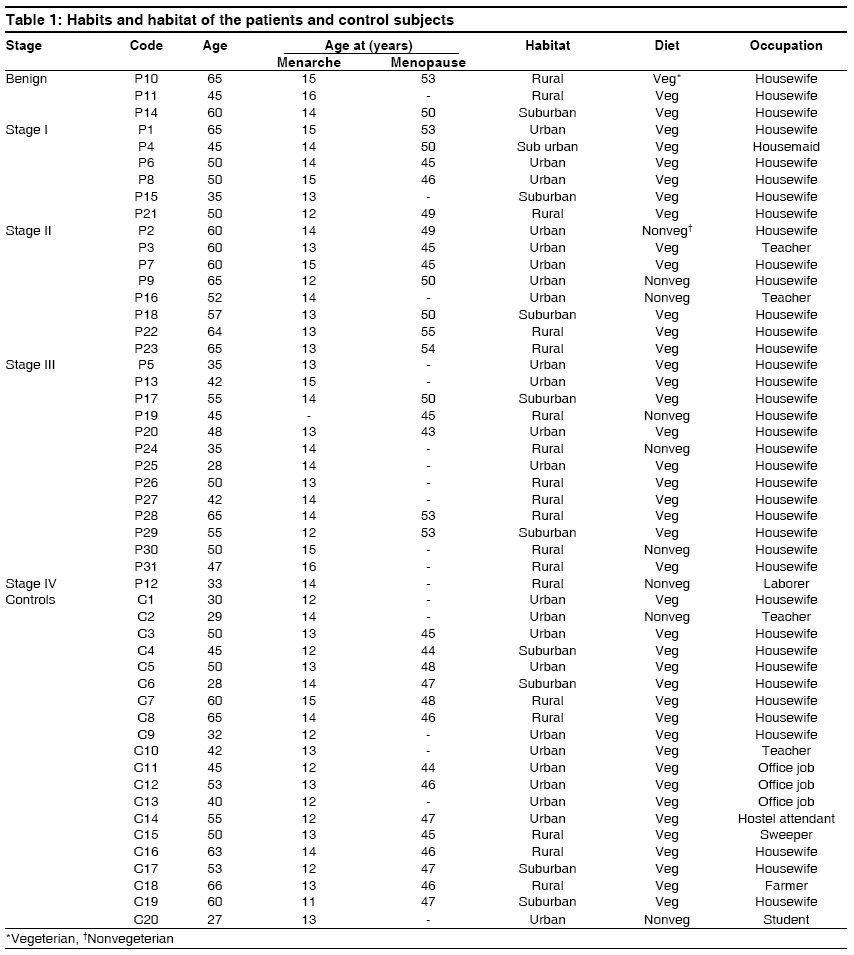
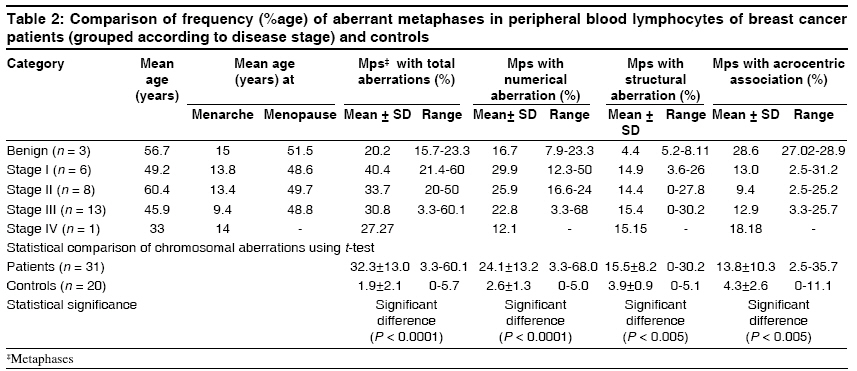
Indian Journal of Human Genetics, Vol. 15, No. 1, January-April, 2009, pp. 13-18 Original Article Chromosomal instability in the lymphocytes of breast cancer patients Harsimran Kaur, Kaur MongaGaganpreet, Nitika Setia, Meena Sudan, Uppal MS, Yamini, Batra A. P. S., Vasudha Sambyal Department of Human Genetics, Guru Nanak Dev University, Amritsar, Punjab-143 005 Code Number: hg09004 DOI: 10.4103/0971-6866.50864 Abstract Genomic instability in the tumor tissue has been correlated with tumor progression. In the present study, chromosomal aberrations (CAs) in peripheral blood lymphocytes (PBLs) of breast tumor patients were studied to assess whether chromosomal instability (CIN) in PBLs correlates with aggressiveness of breast tumor (i.e., disease stage) and has any prognostic utility. Cultured blood lymphocyte metaphases were scored for aberrations in 31 breast cancer patients and 20 healthy age and sex-matched controls. A variety of CAs, including aneuploidy, polyploidy, terminal deletions, acentric fragments, double minutes, chromatid separations, ring chromosome, marker chromosome, chromatid gaps, and breaks were seen in PBLs of the patients. The CAs in patients were higher than in controls. A comparison of the frequency of metaphases with aberrations by grouping the patients according to the stage of advancement of disease did not reveal any consistent pattern of variation in lymphocytic CIN. Neither was any specific chromosomal abnormality found to be associated with the stage of cancer. This might be indicative of the fact that cancer patients have constitutional CIN, which predisposes them to the disease, and this inherent difference in the level of genomic instability might play a role in disease progression and response to treatment.Keywords: Breast cancer, chromosomal aberrations, genomic instability, lymphocytes. Introduction Cancer is a complex disease in which cells with altered gene expression grow abnormally, invade other tissues, and disrupt their normal function. A crucial early event in carcinogenesis is the induction of the genomic instability phenotype, which enables an initiated cell to evolve into a cancer cell by achieving greater proliferative capacity and genetic plasticity to overcome host immunological resistance, localized toxic environment, and suboptimal micronutrient supply. Genomic instability in cancer can be of two types: microsatellite instability (MIN) and chromosomal instability (CIN). MIN tumors exhibit an apparently normal karyotype and have mutations in DNA mismatch repair genes. But, a majority of the tumors exhibit abnormal karyotypes involving either chromosomal rearrangement and/or aneuploidy and are classified as CIN tumors. [1],[2],[3] Various reports indicate a significant increase in the chromosomal aberrations (CAs) in peripheral blood lymphocytes (PBLs) of cancer patients with solid tumors. [4],[5],[7] PBLs of patients with breast cancer and other solid tumors show simple chromosomal lesions that may be stable markers in cancer cells. [8] Hence, it is proposed that lymphocytes may be used as a surrogate tissue model for studying genomic instability in case of solid tumors and the frequency of CAs in PBLs can be used as a predictor of cancer risk. [9],[10],[11],[12] Breast cancer is a major global health problem and the incidence of the disease continues to increase steadily. The frequency of sporadic breast cancer is higher in areas adjoining Amritsar city of Punjab, India (Unpublished data, Rotary Cancer Hospital, Amritsar; personal comunication). In the present study, CAs in PBLs of sporadic breast tumor patients were studied to assess whether CIN in PBLs correlates with aggressiveness of breast tumor, i.e. disease stage, and has any prognostic utility. Materials and Methods Five milliliters of blood sample from 31 cancer patients, 28 with sporadic malignant breast cancer and three with benign breast disease, were collected before surgery from the surgical wards of Sri Guru Ram Das Institute of Medical Sciences and Research, Amritsar (Punjab), after informed consent was obtained. Institutional ethical committee approval was obtained for the study. Relevant information regarding age, symptoms, duration and stage of the disease (TNM classification), habits, habitat, menstrual and reproductive history, occupation, and exposure of the patients to mutagens was recorded on a predesigned questionnaire. Age and sex-matched controls were randomly selected from the general population of Amritsar. Blood samples of 31 breast cancer patients and 20 healthy age and sex-matched controls were cultured in RPMI 1640 medium according to the standard culturing technique, [13] with some modifications. Slides were GTG banded according to the Benn and Perle [14] method. Banded slides were scanned for numerical and structural aberrations. For each subject, 100 clear metaphases were assessed for CAs. Of these, 10 metaphases were karyotyped as per ISCN 2005. The t-test was used to compare the frequency of aberrant metaphases among patients and controls.Results Among the patients, one patient had stage IV disease, 13 had stage III disease, eight were diagnosed at stage II, six had stage I, and three patients had benign disease. The cancer patients were in the age group of 28-65 years. None of the patients had history of early menarche (before the age of 12 years) or late menopause (after 55 years) in postmenopausal patients. 77.4% of the patients (n = 24) consumed vegetarian diet and only 22.5% (n = 7) consumed nonvegetarian food occasionally. All of them had first full-term pregnancy before the age of 30 years. 87.1% (n = 27) of the patients were housewives. Twelve patients (38.7%) belonged to urban area, six (19.3%) of them had suburban habitat, and 13 (42%) belonged to rural areas surrounding Amritsar [Table - 1]. Control subjects were in the age group of 27-66 years. Fifty-five percent (n = 11) of the controls belonged to urban areas, 20% (n = 4) of them were from suburban areas, and 25% (n = 5) belonged to rural area. Most (90%) (n = 18) of them consumed vegetarian diet [Table - 1]. The frequency of aberrant metaphases varied from 3.3 to 60.1% in cultured lymphocytes of patients and from 1.5 to 5.7% in controls [Table - 2]. Stage I patients had aberrant metaphases ranging from 21.4 to 60%. The frequency of aberrant metaphases ranged from 20 to 50% in stage II patients and 3.3 to 60% in stage III and IV patients. Enormous variation was also seen for numerical and structural aberrations among patients with various stages of advancement of disease. A variety of CAs, including aneuploidy, polyploidy, terminal deletions, acentric fragments, double minutes, chromatid separations, ring chromosome and marker chromosome, chromatid gaps, and breaks were seen in PBLs of the patients. Specific CA correlated with stage of cancer was not observed, neither was any particular chromosome found to be involved in aberrations in all the patients. A high frequency of acrocentric associations (D-D, G-G, D-G) was seen in all the patients as compared to controls. The mean value of percent total aberrations in patients was 32.3% and in control subjects was 1.9%. A statistically significant difference in the percentage of aberrant metaphases was seen among patients and controls (t-value = 10.1, P < 0.001). Discussion Genetic instability is a defining feature of human cancer. In the present study, breast cancer patients had a significantly higher percentage of aberrant metaphases as compared with controls. There was a high frequency of numerical as well as structural abnormalities in the cultured lymphocytes of patients, but enormous variation was seen in the level of lymphocytic CIN among the breast cancer patients. The mean of percentage of metaphases with aberrations was 20.2% in patients with benign disease, 40.4% in stage I patients, 33.9% in stage II patients, 30.8% in stage III patients, and 27.3% in stage IV patients. However, the percentage of aberrant metaphases ranged from 15.7 to 23.3% in patients with benign disease, 21.4 to 60% in stage I patients, 20.1 to 50.2% in stage II patients, and 3.3 to 60.1% in stage III patients, suggestive of variability in the underlying genomic composition of these patients. Grouping of patients according to the stage of advancement of disease did not reveal any consistent pattern of variation in lymphocytic CIN [Table - 2], in contrast to tumor tissue where genomic instability has been correlated with tumor progression. Genomic instability has been found to be low in benign and hyperplastic tissues, but dramatically increased in ductal carcinoma and invasive cancer. [15] Frequency of allelic imbalance (or MIN) in tumor tissue has been shown to be significantly correlated with tumor progression in colorectal cancer. [16] In a fluorescent in situ hybridization study of numerical alterations of chromosomes 7, 8, 16, and 17 in 28 ductal carcinoma in situ (DCIS), it was shown that the patterns of aneuploidy in breast tumor tissue may differ according to the tumor grade. [17] This indicated that lymphocytic CIN was an index of inherent instability in the patient′s genome and was not influenced by the disease status, whereas genomic instability of the tumor could be influenced by the patient′s disease status or aggressiveness of tumor. High frequency of aberrations in PBLs of breast cancer patients similar to that seen in tumor tissue has already been reported in several studies. [12],[18],[19],[20] Also, greater than expected infrared-induced genomic instability has been seen in lymphocytes of patients with breast cancer and other solid tumors. [21],[22],[23] Thus, cancer patients probably have constitutional CIN, which participates in cancer predisposition. Aberrations involving specific chromosomes (2, 7, 11, 12, 15, 19, 22, and X) in the lymphocytes of breast cancer patients have been reported in a previous study. [20] Various genes involved in genomic stability and breast tumorigenesis [EP300 (22q13.2), LKB1 (19p13.3), FGFR1 (8p11.2), CHEK2 (22q) and K-ras (12p12)] are located in these regions and might be involved in the variable CIN phenotype. The variable CIN phenotype is due to alterations at different CIN loci. CIN genes are involved in a variety of pathways, including chromosome condensation, sister chromatid cohesion, kinetochore structure and function, microtubule formation, and cell-cycle control. [24] Another interesting observation from the analysis of epidemiological data of the patients was that many of the well-established epidemiological risk factors reported in previous studies on western data (i.e., late age of menopause, early age of menarche, nulliparity, older age at first birth, alcohol consumption, high meat intake, and high socioeconomic status [25],[26] ) did not account for the etiology of the disease in patients in the present study. Early age at menarche (less than 12 years of age) has been associated with a 10-20% increase in breast cancer risk and delayed menopause (after 54 years of age) maximizes the number of ovulatory cycles, leading to increased breast cancer risk. [27],[28],[29] Nulliparity and late age at first birth also contribute toward an increased risk of developing breast cancer. [25] In the present study, most of the patients had a normal reproductive and menstrual history. The age at menarche of the patients varied from 12 to 16 years and age at menopause was between 43 and 55 years. Most of them consumed a vegetarian diet and none of them reported alcohol consumption. Thus, some genetic and environmental factors might be acting synergistically and are responsible for the high incidence of breast cancer in this area. Amritsar has many small-scale industries, such as textile processing, woolen, dyeing, electroplating, pharmaceutical, iron foundaries, pulp and paper mills, steel plants, dairy, and glass and plastic mills, and the area adjoining the city is mainly agricultural land, where the use of pesticides and agricultural chemicals is high. Heavy metal contamination has also been reported in agricultural products, soil, and water in and around Amritsar (www.punjabenvironment.com). In the present study, the patients had much higher CIN than controls. Even patients with benign disease or at stage I had higher CIN than controls. But, the patients had variation in the level of CIN in PBLs with no apparent correlation with disease stage, as a stage I patient had up to 60% aberrant metaphases while a stage II patient had only 3.3% aberrant metaphases. The present study is in agreement with the previous reports on validity of cytogenetic assay for determination of frequency of CAs as a biomarker for cancer risk. [8],[9],[10],[11] Such studies had been subject to criticism due to not accounting for the reverse causality bias, i.e. when the biomarker might be affected by the disease. But, the present study suggests an independence of this biomarker from disease stage. The inherent difference in the level of genomic instability might play a significant role in disease progression, patient tolerance for radiation and antineoplastic agents, and recurrence risk. Breast cancer (BRCA) proteins and their associated molecules (e.g., Fanconi anemia proteins, Ataxia telangiectasia mutated- Ras-associated diabetes (ATM- RAD complex) work in a network of connected biological complexes that encompass virtually all aspects of the cellular response to DNA damage during the S and G2 phases of the cell cycle. [30] Cells lacking these proteins fail to correct endogenous DNA damage during or after DNA synthesis. Individuals with mutation in BRCA or associated proteins show sensitivity to DNA cross-linking agents such as cisplatin and mitomycin C. Determination of the genomic instability level of individual patients before planning therapy may help avoid tissue and cellular damage by radiation and cancer chemotherapy drugs by permitting less-aggressive therapy of the sensitive patients. Acknowledgment Financial assistance in the form of grant from Council for Scientific and Industrial Research, India (grant no. 09/254(0162)/2006-EMR-1) to HK and Punjab State Council for Science and Technology (grant no. SSO/P08/80/1269) to GKM is highly acknowledged. We are grateful to Prof. Dr. Geeta Sharma, Principal SGRDIMSR, Amritsar for allowing access to the patients.References
Copyright 2009 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg09004t1.jpg] [hg09004t2.jpg] |
| |||||||||


{kind=link}
{kind=link}