 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
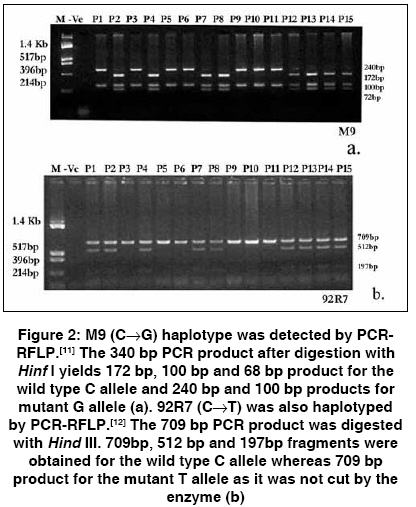
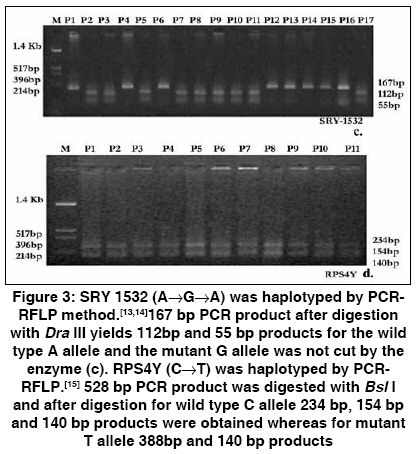
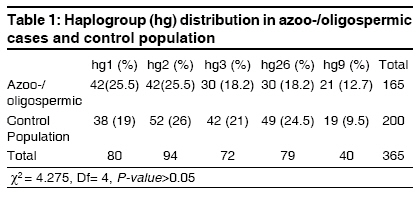
Indian Journal of Human Genetics, Vol. 15, No. 1, January-April, 2009, pp. 19-22 Original Article Y-haplotypes and idiopathic male infertility in an Indian population Singh Kiran, Raman Rajiva Department of Molecular and Human Genetics, Banaras Hindu University, Varanasi Code Number: hg09005 DOI: 10.4103/0971-6866.50865 Abstract Infertility being a multifactorial disorder, both genetic and environmental factors contribute to the etiology of infertile phenotype. Chromosomal anomalies and Y-microdeletion are the established genetic risk factors of male infertility. Y-haplotypes has been found as risk factor for male infertility in certain populations, though in certain others no association has been reported, suggesting a population-specific association of these variations with male infertility. In a case-control study, 165 azoo-/oligospermic patients and 200 controls were haplotyped for certain Y-haplogroups for a possible association with idiopathic male infertility in an Indian population. Analysed Y-haplogroups showed no association with infertile phenotype. Thus this genetic factor is not a risk for infertility in the studied Indian population but that does not rule out the possibility of any of them, to be a risk in other populations.Keywords: Male infertility, single nucleotide polymorphism, Y-haplotypes Introduction The human Y chromosome contains over 60 million nucleotides, and act as a genetic determinant of the male characteristic features. Though rearrangement or sequence variation in these genes is expected to lead to impaired spermatogenesis and reduced sperm count, [1],[2] seldom has a mutation in a single gene been associated with nonobstructive male infertility. On the other hand, the genetic cause of idiopathic azoospermia and oligospermia is predominantly associated with chromosomal aneuploidy, rearrangements, and microdeletions in the AZF region of the Y-chromosome. [3],[4] The lack of inter-chromosomal recombination in larger part of the Y-chromosome facilitates accumulation of a variety of slow mutating binary markers such as SNPs. Variation in their relative frequency in different populations gives rise to diverse chromosomal haplotypes. [5] A few studies have shown an association of certain Y-haplogroups with low sperm count and azoospermia in certain populations which fortifies the idea that selection processes are still active on the Y-chromosome. [1],[6] An association with infertility has also been shown with the common SNP C677T of MTHFR gene in an Indian case-control study. [7] However, similar case-control studies for MTHFR C677T in European population have failed to record any correlation with male infertility. [8],[9],[10] Thus the suggested association of the Y-chromosomal haplogroups, and/or polymorphisms in MTHFR gene with infertility indicates that certain genotypes/haplotypes affect fertility in region-specific manner. The present study is addressed to the possible association of certain Y-haplotypes with infertility in the cases from eastern part of India. The Y-haplogroups chosen are those whose association with infertility has been demonstrated in Japanese and Danish populations. [1],[6] However, the results failed to reveal any association of the haplogroups with infertility in the analysed population, though in the same cohort of cases and controls, C677T in the MTHFR gene had shown a strong association with infertility. Materials and Methods Subjects Y Haplogroup analysis Statistical analysis Results For Y-haplotyping, SNPs M9, 92R7, SRY-1532, RPS4Y and the Indel marker (12f2) were analysed. A parsimony network illustrating the relationships between the analysed haplogroups is shown in [Figure - 4]. The haplogroup frequencies observed in azoo-/oligospermic infertile and fertile control men are summarized in [Table - 1]. Out of the 6 haplogroup (Hg) markers used, only five were present in the studied population, Hg10, defined by RPS4Y711 C→T transition, being absent. [17] The association data as well as the frequency of alleles of different markers between the fertile and the azoo-/oligospermic subjects were subjected to χ2 statistical analysis. The test results revealed no statistically significant difference at the 5% level for both the groups. Similarly, the analysed haplogroups revealed no difference between the case and control samples [Table - 1]. Also, there was no significant association in the distribution of any of the markers (M9, 92R7 and SRY-1532) with the case or the control populations.Discussion Compared with autosomal or mitochondrial DNA, the Y-chromosome shows a relatively higher level of geographic specificity. In the context of male infertility and Y-haplogroup, Hg 26+ shows a risk for infertility in a Danish population. [1] In another report, an association of Hg4 with low sperm count and infertility was found in a Japanese population. [6] However, a reassessment of Kuroki′s Hg 4 data along with other Y chromosome haplogroups (Hg20, 5, 2) from the same Japanese population did not find any association with infertility. [17] Similarly, a study on Italian subpopulations of infertile and control individuals initially indicated an association with specific haplogroups and idiopathic infertile males, but when samples were subdivided according to their origins the putative association between the two groups disappeared. [18] The present report too does not find any haplogroup′s association with infertility. Hg26+, which showed association in the Danish population, had only a minor presence in both groups in the present study. The fact that so far only Hg26+ has shown a clear association suggests that there is need for exploring more haplogroups in more populations, and that a more rigorous analysis of multiple haplogroups may be necessary to derive meaningful conclusions. In this paper we have found no association of infertility with the Y-chromosome haplogroups in an Indian population. Nevertheless, we maintain that such association studies need to be extended in their scope and in diverse populations to get a better perspective of the genotype-environment interaction in this multifactorial disorder. Acknowledgments We are thankful to all the patients and volunteers for providing blood samples and tissue material. Thanks are also due to Dr. S. K. Singh for his help in patient recruitment. Ethical Approval: Written consent of all the participants was obtained and approved by the "Research Ethical Committee" of the Institute of Medical Sciences, Banaras Hindu University, India. Funding: This work was supported by a grant from the Department of Biotechnology, New Delhi, to R. R. and a SRF to Kiran Singh from the CSIR. References
Copyright 2009 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg09005t1.jpg] [hg09005f4.jpg] [hg09005f3.jpg] [hg09005f2.jpg] [hg09005f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}