 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
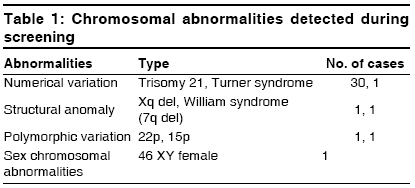
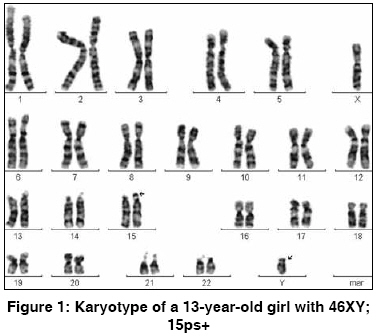
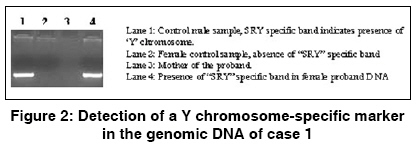
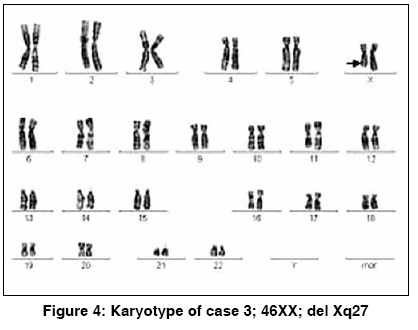
Indian Journal of Human Genetics, Vol. 15, No. 1, January-April, 2009, pp. 28-31 Brief Report Chromosomal abnormalities associated with mental retardation in female subjects Dutta Samikshan, Shaw Jyoti, Sinha Swagata, Mukhopadhyay Kanchan Manovikas Biomedical Research and Diagnostic Centre, 482, Madudah, Plot I-24, Sec.-J, E.M. Bypass, Kolkata - 700 107 Code Number: hg09007 DOI: 10.4103/0971-6866.50867 Abstract Chromosomal abnormalities are thought to be the most common cause of mental retardation (MR). However, apart from a few selected types with typical aneuploidy, like Downs syndrome, Klinefelter syndrome, Turner syndrome, etc., the frequency of detectable chromosomal abnormalities in association with idiopathic MR is very low. In this study, we have investigated chromosomal abnormalities in female MR subjects (n = 150) by high-resolution GTG banding. Of them, 30 cases were diagnosed as Downs syndrome. Among the remaining (n = 120), chromosomal abnormalities/marked polymorphisms were detectable in only three MR cases (0.025).Keywords: Chromosomal abnormalities, GTG-banding, karyotype, MR Introduction Chromosomal abnormalities that alter developmental gene expression are the most common cause of mental retardation (MR). [1] Overall, ~10% of MR cases suffer from chromosomal abnormalities. [2] In depth analysis has shown that nearly 40% severe MR cases suffer from some form of chromosomal abnormalities whereas only about 10% mild MR cases show detectable chromosomal aberrations. [3] Telomeric regions of chromosomes are the most gene-rich regions and any deletion or alteration in this region had been reported to account for nearly 2.5% MR, with or without dysmorphic features. [4] This percentage varies greatly between 2 and 29% (overall 6%). These regions are also highly susceptible to meiotic recombination and may be responsible for idiopathic MR (IMR). [5] Studies have also shown a male preponderance for all types of MR, with males being 1.6-1.7-times more vulnerable as compared with females, [6],[7] which may be attributed to X-linked disorders. However, till date, not many studies have been carried out on the female MR probands. The present investigation was aimed at studying chromosomal abnormalities in female IMR subjects.Materials and Methods Heparinized blood sample was collected for lymphocyte culture from 150 female MR cases after obtaining informed written consent for participation. [8] Plasma was added to an RPMI 1640 medium supplemented with 10% fetal bovine serum and phytohemagglutinin and was incubated for 69 h at 37 o C in a CO 2 incubator (Heraeus, Kendro Laboratory Products GmbH, Germany) followed by metaphase arrest with colcemid (N-deacetyl-N-methylcolchicine). Cells were harvested after 45 min of colcemid treatment and subjected to hypotonic shock with 0.075 M KCl followed by fixation of the cell pellet with chilled Carnoy′s fixative (methanol:aetic acid, 3:1). Later, GTG-banding analysis [9] of the fixed cells on glass slides was carried out with controlled trypsin digestion and Geimsa staining. Cells were visualized under the oil immersion lens of a Zeiss Axioskop2 plus microscope, Carl Zeiss India Pvt. Ltd. and at least 50 well-spread metaphase plates were analyzed with the karyoimager software. DNA was isolated from ethylenediaminetetraacetic acid-treated blood samples and polymerase chain reaction (PCR) was carried out with SRY-specific primers for detection of Y chromosome (details available on request). Results Of the 150 female MR probands recruited, highest frequency (0.2) of chromosomal abnormalities was observed for Downs syndrome (with trisomy 21), with only few cases of other abnormalities being reported [Table - 1]. Of the remaining 120 cases, 64 were identified as IMR, with a very low frequency of detectable chromosomal abnormalities (0.046), and 56 cases were diagnosed as MR, with records of birth asphyxia, epileptic seizure, cerebral palsy, William syndrome (del 7q), Turner syndrome (XO), etc. The IMR cases showing abnormal karyotypes are discussed below. Case Reports Case 1 High-resolution banding analysis revealed an apparent male karyotype of 46, XY with a polymorphic variation of enlarged satellites in the 15 ′p′ arm (15ps+): the satellites on one homologue of chromosome 15 were enlarged [Figure - 1]. This polymorphism was also detectable in the mother. Presence of the Y chromosome, or at least a part of it, was confirmed by PCR using SRY gene-specific primers [Figure - 2]. Her testosterone level was 1.3 nmol/l. Because her testosterone level was within normal limits, whether this "Y" chromosome contributed to any major phenotype has not yet been resolved. Case 2 In this case, the satellite on one homologue of chromosome 22 was prominent (22ps+), which was also fFound to be present in her mother [Figure - 3]. Although her mother had a normal IQ, the proband had a low IQ (< 70) and delayed brain development. Case 3 In the proband, a deletion in one of the X chromosomes, Xq27, was observed [Figure - 4]. The deletion of the terminal X region could be responsible for altered gene expression leading to virilization in the patient. On the other hand, this might be due to inactivation of Xq in the intact X chromosome (one without deletion). Discussion As was suggested previously, interpretation of subtelomeric rearrangements or other chromosomal abnormalities in MR individuals is often complicated by the fact that many deletions or duplications appear to be benign in familial variants while associated with a particular phenotype in an affected individual. [5] The variation in the expression pattern observed in the present investigation between the probands and their mothers also supports the above notion. Epigenetic regulation [10] or environmental factors may give rise to such differences in phenotypic expression. Other than these three, no other chromosomal abnormality was noted in the cases studied. It may be assumed that minute telomeric or subtelomeric changes were overlooked by GTG-banding analysis. More detailed analysis employing special techniques like subtelomere fluorescent in situ hybridization, comparative genomic hybridization, or spectral karyotyping may help in determining the actual frequency of chromosomal abnormalities in the MR cases. References
Copyright 2009 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg09007t1.jpg] [hg09007f4.jpg] [hg09007f3.jpg] [hg09007f1.jpg] [hg09007f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}