 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
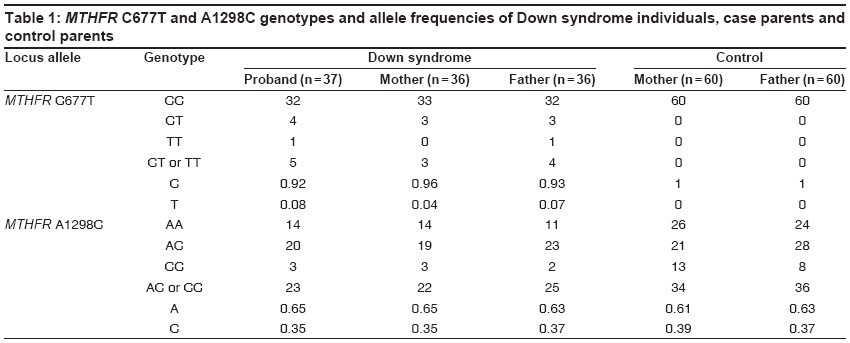
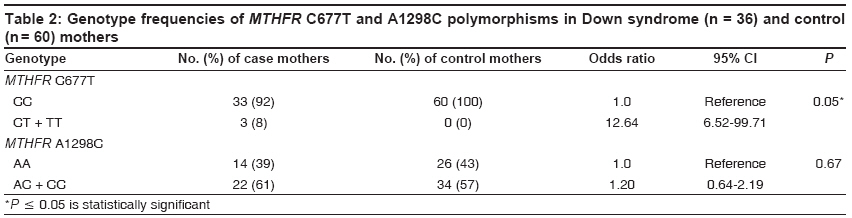
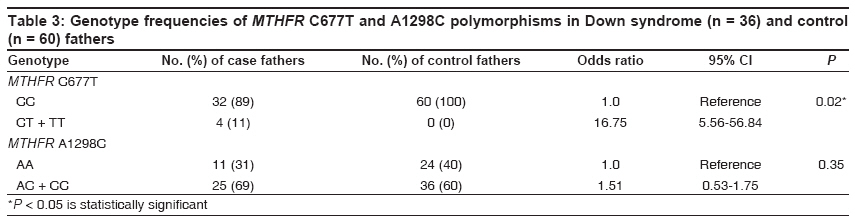
Indian Journal of Human Genetics, Vol. 15, No. 2, May-August, 2009, pp. 60-64 Original Article MTHFR Gene variants C677T, A1298C and association with Down syndrome: A case-control study from South India Cyril Cyrus, Rai Padmalatha, Chandra N, Gopinath PM, Satyamoorthy K Department of Biotechnology, Manipal Life Science Center, Manipal University, Manipal - 576 104 Code Number: hg09015 DOI: 10.4103/0971-6866.55217 Abstract Background: The 5,10-methylenetetrahydrofolate reductase ( MTHFR ) polymorphisms and low folate levels are associated with inhibition of DNA methyltransferase and consequently DNA hypomethylation. The expanding spectrum of common conditions linked with MTHFR polymorphisms includes certain adverse birth outcome, pregnancy complications, cancers, adult cardiovascular diseases and psychiatric disorders, with several of these associations remaining still controversial. Trisomy 21 or Down syndrome (DS) is the most common genetic cause of mental retardation. It stems predominantly from the failure of chromosome 21 to segregate normally during meiosis. Despite substantial research, the molecular mechanisms underlying non-disjunction leading to trisomy 21 are poorly understood.Materials and Methods: Two common variants C677T and A1298C of the MTHFR gene were screened in 36 parents with DS children and 60 healthy couples from Tamil Nadu and Karnataka. The MTHFR genotypes were studied by RFLP analysis of PCR-amplified products and confirmed by sequencing. Results: The CT genotype was seen in three each (8.3%) of case mothers and fathers. One case father showed TT genotype. All the control individuals exhibited the wild type CC genotype. A similar frequency for the uncommon allele C of the second polymorphism was recorded in case mothers (0.35) and fathers (0.37) in comparison with the control mothers (0.39) and fathers (0.37). Conclusion: This first report on MTHFR C677T and A1298C polymorphisms in trisomy 21 parents from south Indian population revealed that MTHFR 677CT polymorphism was associated with a risk for Down syndrome. Keywords: Down syndrome, MTHFR polymorphisms, nondisjunction, trisomy 21 Introduction Gene-nutrient interactions associated with abnormal folate metabolism and DNA hypomethylation were suggested to increase the risk of chromosomal non-disjunction.[1] A mildly elevated plasma homocysteine level and a 2.6-fold increase in the frequency of the MTHFR 677 C?T polymorphism were observed in the mothers of Down syndrome (DS) patients. Several studies with conflicting results have been published on polymorphisms in genes involved in folate metabolism in mothers of DS children. [2],[3],[4],[5],[6],[7],[8] However, there are only few reports on MTHFR polymorphisms from the Indian subcontinent, in particular four, on their role in non-disjunction among DS mothers.[7],[9],[10],[11] The present case-control study aimed to evaluate the association between DS and MTHFR polymorphisms among Indians hailing from Tamil Nadu and Karnataka and this is the first report. Materials and Methods EDTA-anticoagulated blood was collected from 37 children with DS including a pair of sibs and their parents. These children were selected after cytological demonstration of free trisomy 21. The study group included 25 males and 12 females and belonged to the age group of 1/12-16 years. These children were registered at the Department of Medical Genetics, Institute of Child Health and Hospital for Children, Egmore, Chennai or at Kasturba hospital, Manipal. Peripheral blood was also obtained from 60 healthy couples who served as controls. They did not experience any miscarriage or have an affected child. Informed consent for participation in the study was obtained from all the individuals and this study was approved by the Institutional Ethics Committee. Genomic DNA was extracted from these samples following the salting out method of Miller et al.[12] PCR amplification of exon 4 of MTHFR gene was performed in a programmable thermal cycler for C677T mutation analysis. The sequences of the forward and reverse primers were: 5′TGAAGGAGAAGGTGTCTGCGGGA3′ and 5′AGGACGGTGCGGTGAGAG TG3′ respectively. The PCR reactions were carried out in a total volume of 30 µl. It contained 15.7 µl of milli Q water, 3.0 µl of 10X PCR buffer, 3.0 µl of MgCl2 (2 mM), 1.5 µl each of forward (0.5 mM) and reverse primer (0.5 mM), 3.0 µl dNTP mix (200 mM), 2.0 µl of genomic DNA (20 pmol) and 0.3 µl Taq DNA polymerase (in vitro gen). The mixture was subjected to amplification with initial denaturation at 94°C for four minutes, followed by 30 cycles of denaturation at 94°C for 30 sec, annealing at 62°C for 30 sec and extension at 72°C for 40 sec where the extension step in 30th cycle was for five minutes. The amplified 198bp fragment was digested with Hinf I at 37°C for 4 h. The digested products were visualized after separation by gel electrophoresis in two per cent agarose gel with ØX ladder. For A1298C mutation analysis, PCR amplification of exon 7 of MTHFR gene was done using primers 5′GGTCCCCACTTCCAGCATC3′ and 5′GCAAGTCCCCCAAGGAGG3′. Total volume of the reaction mix was 30 µl. The conditions for PCR included an initial denaturation at 94°C for four minutes minutes, followed by 30 cycles of denaturation at 94°C for 30 sec, annealing at 62°C for 30 sec and extension at 72°C for 40 sec. The final cycle included an extension at 72°C for five minutes. PCR amplification resulted in a 145bp product and this was digested overnight with Mbo II at 37°C. The digested products were electrophoresed in two per cent agarose gel with ØX ladder. Sequencing of each of the three genotypes in the two MTHFR polymorphisms was done using automatic DNA sequencer (Applied Biosystems 3130, USA). Genotype and allele frequencies were calculated under assumption of Hardy-Weinberg equilibrium. Statistical analysis was done using Stats Direct software package. Fisher Exact test was applied where values were less than ten. Values of P less than or equal to 0.05 were considered to be significant. Odds ratio was used as an estimate of relative risk. Results The mean maternal age at the time of birth of DS child was 25.81 plus/minus 5.53y (range: 18-37). Fifteen mothers (41.67%) were under 25y, 15 (41.67%) were between 25 and 30y and 6 (16.66%) were older than 30y. The birth order of the proband ranged from first to fifth in the six older mothers. Similarly, the mean paternal age was 31.72 plus/minus 6.94y (range: 21-55). Fifteen (41.67%) were under 30y, 12 (33.33%) were between 30 and 35y and 9 (25%) were above 35 years of age. The mean age for Down syndrome children was 4.94 plus/minus 3.47y (range: one month-16y). In the control group, 38 (63%) mothers were below 25y and 16 (27%) were aged between 25 and 30y. The remaining six were above 30y. The mean maternal age was 24.5 plus/minus 7.36 years (range: 14-32). Twenty eight (47%) fathers were below 30y, 24 (40%) were between the age of 30-35 years and eight were above 35 years. The mean paternal age was 30.93 plus/minus 6.97 years (range: 21-34). A majority of the couples (35) had two children, while 11 of them had a single child. Three and four children were seen in 11 and two families respectively. Only a single couple was reported to have six children. The C-to-T transition was detected by cleavage of the 198bp fragment into 175bp and 23bp fragments. Three case mothers and three fathers showed a CT genotype while one case father was a homozygous TT. Control parents lacked the uncommon T allele [Table - 1]. The T allele frequency was statistically significant in the case parents when compared with the control parents [Table - 2]. The MTHFR A-to-C transversion abolishes a restriction site of Mbo II and is detected by merger of the 79bp and 29bp bands into a 108bp band. The heterozygous AC genotype was found in 52.8 and 35 percent of the case and control mothers respectively. The corresponding values were 63.9 and 46.7 percent in the case and control fathers respectively [Table - 1]. It was of interest to observe about three-fold increase in the frequency of the homozygous CC genotype in control parents in comparison to case parents. However, the allele frequencies were almost similar for the two groups [Table - 3]. Discussion Several studies have shown a relatively high frequency of T allele in mothers of children with DS and have suggested it to be a risk factor for non-disjunction.[1],[2],[7],[8],[13] Heterozygous and homozygous genotype frequencies (CT and TT) were higher among Egyptian case mothers than controls with an odds ratio of 2.34 and 2.75 respectively.[13] However, no association could be demonstrated in few other reports.[3],[4],[11],[14],[15] In the largest case-control study between 152 Turkish mothers of DS children and 91 control mothers, Boduroglu et al.[14] found an insignificant difference in 677C greater than T and 1298A greater than C MTHFR polymorphisms (P is equal to 0.28). Kohli et al.[10] also observed lack of an association in their study on north Indian DS mothers while a case-control study on Indian mothers of DS children from a north-eastern State showed a 7.6-fold increase in the frequency of TT genotype in the case mothers than in the controls.[7] Dutta et al.[9] investigated 75 DS families from West Bengal and observed that the allelic frequencies did not differ in parents of DS patients as compared to controls. There was no preferential transmission of T allele also. On the other hand, the present study revealed a significant difference in the T allele frequency between case and control parents (P 0.05). The minor allele frequencies in case mothers and fathers were 4.17% and 6.94% respectively. However, females were found to have a higher T allele frequency than males in a large study by Devi et al.[16] Five out of 195 females were homozygous for TT whereas none of the 225 males examined showed TT genotype. The frequency of the A1298C homozygous mutant genotype was higher among the control parents in the present study. Contrary to this finding, Rai et al.[7] reported an increased frequency of the CC genotype among case mothers. Meguid et al.[13] also noticed that the mutant genotype was significantly more common in case mothers than in controls (OR is equal to 31.5) indicating a greater genetic impact of this polymorphism. Micronutrient intake was suggested to influence the effects of polymorphisms in genes involved in the folate pathway and to explain the conflicting results.[17] Wilcken et al.[18] studied geographical and ethnic variation of the MTHFR 677C?T allele in 7130 newborns from 16 areas in the Americas, Europe, Russia, China and Australia. They showed that the TT genotype frequency was particularly common in Northern China (20%), Southern Italy (26%) and Mexico (32%) while it was low among the newborns of African ancestry. A very low frequency was also reported in African Indians (seven per cent) and Indian Asians (three per cent). [19],[ 20] Concordant results were observed in reports from the Indian subcontinent.[16],[21],[22],[23] Absence of T allele of C677T in 120 control individuals in the present study was similar to that of an earlier report on 36 subjects from West Bengal.[24] Angeline et al.[23] found the frequency of 677TT among Tamilians to be 1.38% (1/72) and that of 677CT heterozygotes as 18.1% while the frequencies of 1298AC and 1298CC genotypes were 47.2% and 15.3% respectively. The frequencies for the T allele of C677T and for the C allele of A1298C in 30 control individuals were 0.17 and 0.45 respectively.[11] This study also showed a higher frequency of 1298AC (58.3%) than 677CT (8.3%) genotype. The prevalence of A1298C polymorphism was nine per cent in Canada and Netherlands, while it was 13.8%, 17% and 41.1% in populations from Germany, China and Brazil respectively.[25] On the other hand, its prevalence was 19.46% in Indian populations selected on the basis of their linguistic lineage and geographical location, which was higher than that in the Caucasian (9.4%) and Japanese (1.6%) populations.[24] In conclusion, a search for the etiology of chromosome 21 non-disjunction is of great importance. The frequency of 677CT and not 1298AC genotype among mothers of DS children in comparison with control mothers in this primary study from South India was significantly different. The investigation when extended over a larger sample size including determination of polymorphisms of other genes involved in the folate pathway could be more informative. The combined presence of these two polymorphisms was shown to be associated with a greater risk of DS[2],[6],[8],[26] Different ethnic populations must be studied to determine the differences in allelic frequencies in order to evaluate their role as risk factors in the etiology of DS. References
Copyright 2009 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg09015t1.jpg] [hg09015t3.jpg] [hg09015t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}