 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
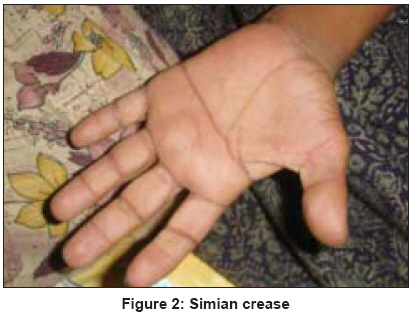
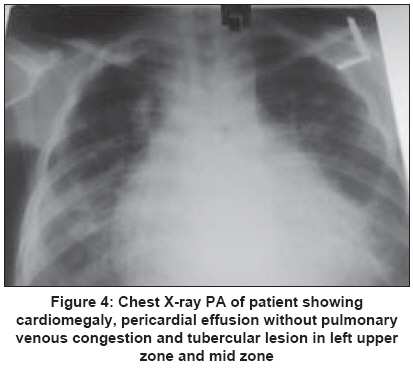
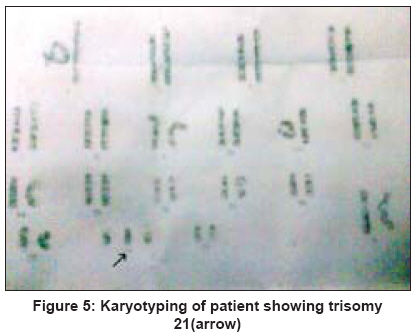
Indian Journal of Human Genetics, Vol. 15, No. 2, May-August, 2009, pp. 72-74 Case Report Down's syndrome and cardiac tamponade with pulmonary tuberculosis in adults Verma SK, Sodhi R Department of Pulmonary Medicine, Chhatrapati Sahuji Maharaj Medical University (erstwhile King George's Medical University), Lucknow, Uttar Pradesh Code Number: hg09017 DOI: 10.4103/0971-6866.55219 Abstract We describe a combination case of Down's syndrome and Cardiac Tamponade with Pulmonary Tuberculosis in an adult patient.Keywords: Cardiac Tamponade, Down′s syndrome, Pulmonary Tuberculosis Introduction A 20-year-old girl of Down′s syndrome presented with Cardiac Tamponade and Pulmonary Tuberculosis (on CAT II) to our department. Literature survey, to the best of our knowledge, revealed that such a condition, in combination, has not been seen till now. Hence we report this case. Case Report A 20-year-old female was referred to us as with the history of recurrent bouts of cyanosis, abdominal swelling and pedal edema with Pulmonary Tuberculosis. Her mother was 40 and father 44 when she was born. Physical examination showed features of Down syndrome (Mongoloid slant of eyes, increased epicanthal distance, bulging forehead, flat occiput, low set ears, protruding tongue [Figure - 1], simian crease [Figure - 2], sandal gap in toe [Figure - 3], protruding belly, hypotonia and mental retardation.) with a slow pulse rate, distant cardiac sounds and absent apex beat. She had normal jugular venous pressure without pulsus paradoxus. She had a history of anti-tuberculosis treatment for six months under CAT I RNTCP around one year back. Routine blood investigations were normal. Sputum for acid fast bacilli was positive two months back. Chest X-ray showed a tubercular lesion in left upper zone and mid zone with cardiomegaly without pulmonary venous congestion [Figure - 4]. The ECG showed QRS microvoltage and flattened P and T segments. Her thyroid function test was normal. Her I.Q. was only 25, thereby classifying her as severe mental retardation (M.R). Ophthalmologic examination was normal. Karyotyping was done and it confirmed that it was a case of trisomy 21 [Figure - 5]. On echocardiography, it was found that patient had pericardial effusion of tamponade physiology also. We advised pericardiocentesis but patient′s attendants did not give consent for the procedure. She was started on diuretics to which she responded. She was discharged in stable condition on CAT II under RNTCP and diuretics. Discussion Down syndrome (DS) is a chromosomal disorder caused by the presence of all or part of an extra 21 st chromosome. It is named after John Langdon Down, the British doctor who described the syndrome in 1866. [1] The condition is characterized by a combination of major and minor differences in structure. Often DS is associated with some impairment of cognitive ability and physical growth as well as facial appearance. Individuals with DS tend to have a lower than average cognitive ability, often ranging from mild to moderate developmental disabilities. [2] A small number have severe to profound mental disability. The incidence of DS is estimated at 1 per 800 to 1,000 births, although these statistics are heavily influenced by the age of the mother. [2] Individuals with DS may have some or all of the following physical characteristics: Oblique eye fissures with epicanthic skin folds on the inner corner of the eyes, muscle hypotonia (poor muscle tone), a flat nasal bridge, a single palmar fold, [3] a protruding tongue (due to small oral cavity, and an enlarged tongue near the tonsils), a short neck, white spots on the iris known as Brushfield spots, excessive joint laxity including atlanto-axial instability, congenital heart defects [4] excessive space between large toe and second toe, a single flexion furrow of the fifth finger, and a higher number of ulnar loop dermatoglyphs. Most individuals with DS have mental retardation in the mild (IQ 50-70) to moderate (IQ 35-50) range, with individuals having Mosaic DS typically 10-30 points higher. In addition, individuals with DS can have serious abnormalities affecting any body system. They also may have a broad head and a very round face. Maternal age influences the chances of conceiving a baby with DS. At maternal age 20 to 24, the probability is one in 1562; at age 35 to 39 the probability is one in 214, and above age 45 the probability is one in 19 [5] Recent data also suggest that paternal age, especially beyond 42, also increases the risk of DS manifesting in pregnancies in older mothers. Trisomy 21 (47,XX,+21) is caused by a meiotic non- disjunction event. With non-disjunction, a gamete ( i.e. , a sperm or egg cell) is produced with an extra copy of chromosome 21; the gamete thus has 24 chromosomes. When combined with a normal gamete from the other parent, the embryo now has 47 chromosomes, with three copies of chromosome 21. Trisomy 21 is the cause of approximately 95% of observed DS, with 88% coming from non-disjunction in the maternal gamete and eight per cent coming from non-disjunction in the paternal gamete. We also discovered pericardial effusion and early cardiac tamponade in our patient. This is an uncommon presentation or generally a complication of hypothyroidism in children. [6] Excluding neonates and children with DS several series have reported pericardial effusions in 50-73% of paediatric patients with hypothyroidism, but none of these series describes patients with symptomatic pericardial effusions or tamponade. Even in adults, most cases of pericardial effusion associated with hypothyroidism do not cause hemodynamic compromise, although tamponade has been reported in the elderly. Effusions develop due to an increased capillary leak of albumin in hypothyroid patients, which can lead to a slow build-up of protein-rich fluid in the pericardial space. [7] Regular evaluation of thyroid function tests is important in DS. Treatment for pericardial effusions associated with hypothyroidism usually involves oral L-thyroxin replacement with resolution of the effusion occurring at 2-12 months. [8] Pericardiocentesis was the usual treatment for effusions with hemodynamic compromise, and there are no reports of using intravenous thyroxin.[9] Levy and colleagues reported on a series of 204 adults with pericardial effusion. Of the 20 patients with thyroid-related effusions, only five were suspected clinically to have a thyroid disorder without the aid of laboratory tests. [10] In conclusion, laboratory screening for hypothyroidism in children as well as adults presenting with apparent idiopathic pericardial effusions may identify occult cases of hypothyroidism. Patients of Down′s have about a 12-fold increased risk of infectious diseases, especially pneumonia, because of impaired cellular immunity. No data till date has commented about any change in prevalence of tuberculosis in such patients. We continued CAT II under RNTCP in this patient and she improved with the treatment. References
Copyright 2009 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg09017f3.jpg] [hg09017f2.jpg] [hg09017f4.jpg] [hg09017f5.jpg] [hg09017f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}