 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
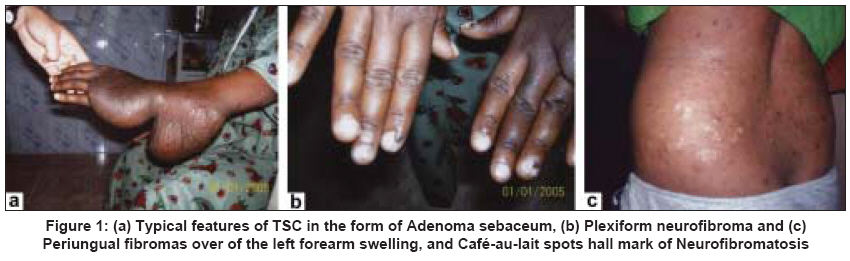
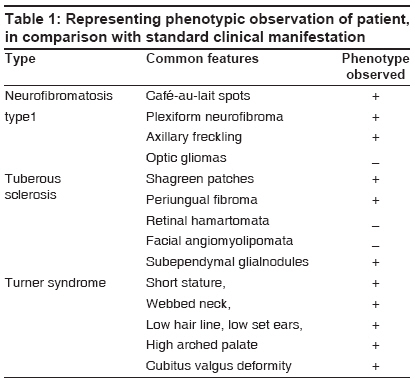
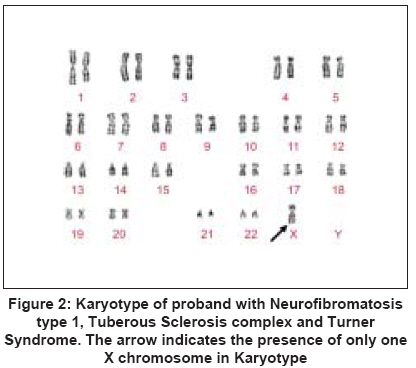
Indian Journal of Human Genetics, Vol. 15, No. 2, May-August, 2009, pp. 75-77 Case Report Rare association of turner syndrome with neurofibromatosis type 1 and tuberous sclerosis complex Suttur MaliniS, Mysore SavithaR, Krishnamurthy Balasundaram, Nallur RamachandraB Department of Studies in Zoology, Human Genetics Laboratory, University of Mysore, Manasagangothri, Mysore - 570 006 Code Number: hg09018 DOI: 10.4103/0971-6866.55220 Abstract We report a rare association of Turner syndrome with both Neurofibromatosis type I and Tuberous Sclerosis. The patient had XO karyotype with Turners stigmata and also had features of Neurofibromatosis 1 in the form of significant cafe-au-lait spots and Plexiform neurofibroma along with typical features of Tuberous Sclerosis complex. Pedigree analysis revealed that the elder brother of the proband in the family also suffered from Tuberous Sclerosis without the manifestation of Neurofibromatosis or any other genetic disorders. We hypothesize that these associations could be due to new independent mutations and also increased maternal and paternal age in a pre-disposition of Turner syndrome.Keywords: India, Neurofibromatosis type I, rare condition, Turner Syndrome, Tuberous Sclerosis Introduction Many common chronic diseases with adult onset show familial aggregation that usually does not follow Mendelian patterns but appears to be caused by an unknown number of multiple genes, usually interacting with various environmental factors. [1] Such conditions include coronary heart disease, hypertension, diabetes, obesity, various cancers, Alzheimer′s disease, Parkinson′s disease and others. In all such diseases, only a small fraction of affected individuals owes its origin to a single mutant gene transmitted by Mendelian inheritance with characteristic transmission. [2] These genetically exceptional families often have an earlier age of onset and have more severe clinical manifestations. So far, success in understanding "complex" diseases has been obtained most in the case of rare monogenic subtypes. Although the result on genetic mechanisms of majority of complex diseases is limited, several chromosomal sites of gene localization have often been reported. We discuss a rare association of Turner syndrome with both Neurofibromatosis type I and Tuberous Sclerosis. Case Report A 20-year-old Turner syndrome (TS) patient with Neurofibromatosis 1 (NF1) and Tuberous sclerosis complex (TSC) was apparently normal till five years of age. She later started developing small skin lesions of the size of pin head over the face which gradually increased in size and number. There was also a swelling over the left forearm, about the size of a marble, which gradually increased to attain the size as shown in [Figure - 1]a. The developmental milestones were within normal limits and the patient had attained menarche at 12 years of age with regular menstrual cycles with no history of seizures. [Table - 1] presents the phenotypic observation of the patient, in comparison with standard clinical manifestation. The expression level varies for all three disease conditions. Clinical investigations revealed that the girl had typical features of TSC in the form of Adenoma Sebaceum, Plexiform Neurofibroma Shagreen patch and Periungual Fibromas [Figure - 1]a and b and multiple Cafι-au-lait spots ranging in size from 1.5cm to 4cm scattered all over the body confirmed NF1 [Figure - 1]c. Along with NF 1 and TSC, Turner features were evident with short stature, webbing of neck, low hair line, low set ears, high arched palate and cubitus valgus deformity. About 10-20% of Turner syndrome girls had spontaneous breast development and a small percentage may have menstrual periods. Pregnancies have been reported for spontaneously menstruating patients. [3] The patient studied had also shown menstruation regularly with normal breast development, normal uterus and ovaries in pelvic ultrasound. Chromosomal analysis of the proband was carried out on peripheral blood lymphocyte culture by using the standard protocol of Seabright. [4] with slight modifications. G-banded metaphases were screened by using a Leica DMRA2 research microscope. A total of 100 well banded metaphase plates were analyzed and karyotyped according to the International System for Human Cytogenetic Nomenclature-2005. Chromosome analysis of the patient confirmed with 45, XO Karyotype [Figure - 2]. An informed consent was obtained from the affected family members, before their inclusion in the study. Pedigree of the proband family revealed that there was no parental consanguinity [Figure - 3]. At the conception of the proband, the ages of the mother and father were 45 and 50 years respectively. There was no history of miscarriage or birth defects but her elder brother also had similar skin lesions over the face, which appeared at the age of seven years with Adenoma Sebaceum, Shagreen patch revealed the appearance of TSC. Discussion There are cases reported on the association with NF 1 and TS. [5] and also NF 1 with TSC. [6] However, the association of NF 1, TSC and Turner Syndrome has not been reported so for to our knowledge. It is well known that NF1 and TSC are autosomal, dominant diseases. In our study, none of the parents and grandparents of the proband showed neither NF1 nor TSC but only one of the sibs of the proband manifested TSC. Therefore, one can surmise that both of these diseases caused due to new independent spontaneous mutations in proband and her elder brother. The possible risk factors for Turner syndrome could be increased maternal and paternal age. [7] As the woman age advances, the reproductive system exhibit changes like accumulation of environmental damage, reduced efficiency of DNA repair, increased genomic instability, genetic factors, hormonal influences, suppressed apoptosis, or decreased effectiveness of antioxidants and micronutrients. This leads to a sub-optimal resumption of Meiosis I and Meiosis II, a change in ovarian functioning due to sub-optimal degradation of uterine environment, which are needed for proper meiotic segregation in the germ cells. [8],[9] The elucidation of genetic risk factors for complex diseases will allow development of susceptibility testing for disease prediction. [10] Unlike prediction of genetic risk in most "single gene" diseases prediction in complex disease will usually be probabilistic by providing a range of risks. Such testing will be particularly important for high risk individuals to prevent by diet, drugs, and/or lifestyle changes which will reduce the risk of these diseases. Acknowledgment The authors thank doctors, patient and patients′ family in Cheluvamba Hospital, Mysore medical college and also Chairman, DOS in Zoology, University of Mysore, Mysore, for providing the facility to carry out this work. References
Copyright 2009 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg09018f1.jpg] [hg09018f2.jpg] [hg09018t1.jpg] [hg09018f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}