 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Human Genetics, Vol. 15, No. 2, May-August, 2009, pp. 78-83 Review Article Drugs impact on CYP-450 enzyme family: A pharmacogenetical study of response variation Kalra Kapil, Jarmal Garima, Mishra Neeti Department of Pharmaceutical Chemistry, Kanak Manjari Institute of Pharmaceutical Sciences, Rourkela, Orissa Code Number: hg09019 DOI: 10.4103/0971-6866.55221 Abstract Pharmacogenetics is the study of genetic basis in the individual response to drugs. A thorough knowledge of this will lead to a future where tailor-made drugs, suiting an individual, can be used. Scandinavian countries have been known for wide usage of pharmacogenetics and the most widely used application is for genotyping CYP2D6 in treating psychiatric illness. The CYP-450 enzyme, a super family of microsomal drug-metabolizing enzymes, is the most important of enzymes that catalyzes phase-I drug metabolism reaction. CYP2D6 is a member of this family and it has been most intensively studied and the best example of pharmacogenetics variation in drug metabolism. Neuro-transmitter and drug acting CNS viz. codeine, dextromethorphan, metoprolol and tryptyline etc. are well metabolized by this enzyme. Thus, CYP2D6 is one of the most important and responsible enzymes which regulates bioavailability and metabolism of drug. Presently 75 alleles of CYP2D6 have been described which are responsible for variance of metabolism and toxicity of drugs. Thus, by determining variance of CYP2D6 using molecular approaches viz., PCR, real-time PCR, DNA micro-array and molecular docking can determine the adverse effects, drug toxicity, bioavailability and therapeutic potential of new drug.Keywords: CYP2D6, pharmacogenetics, single neucleotide polymorphismneucleotide polymorphism Introduction A person′s environment, diet and overall health can influence how s/he responds to medicines. Genes are another factor which determining a person′s response to drugs. Pharmacogenetics aims to understand the role of a person′s genetic make-up play in the good effects and side-effects of a medicine in a person′s body. A thorough knowledge of this will lead to a future where tailor-made drugs, suited for an individual, can be used. Concurrently, wide usage of Pharmacogentics is seen in the Scandinavians Countries and the most widely used application is for genotyping CYP2D6 when treating psychiatric illness. Genetic variation contributes to inter-patient differences in drug response. Such variations may occur for drug metabolism, drug transporter and drug target proteins. Most of the variations occurring in the human genome are single nucleotide polymorphism (SNPs) with an occurrence rate of at least one every 1000 base pairs. Genetic Polymorphism may cause an alteration in the efficacy of a drug or its toxicity. Genes contain instructions for making proteins, including proteins which interact with drugs. Any change in a gene can result in changes in the associated protein involved i.e, an enzyme of dug metabolism. Individuals get one copy of a gene from each parent, but each of those copies may have a change or mutation. Mutation can result in production of an enzyme with reduced function or no enzyme may be produced at all. Depending on whether a Person has 0, 1 or 2 normal copies of genes, he or she may be grouped as poor, intermediate or rapid metabolizer. The less normal copies a person has, the poorer the metabolism, and hence, higher blood levels of the drug. This may result in greater effectiveness or more likely greater side effects. History Looking back, the first pharmacogentics trait to be observed was - "taste blindness" to a chemical called Phenylthiourea (PTU). Individuals with a certain gene profile were unable to taste PTU, while others could.This hereditary chemical insensitivity led researchers to understand the genetic differences between races. Mankind has known genetic sensitivity to various substances since time immemorial which can be corroborated by the fact that susceptibility to alcohol by certain ethnic groups was well known 100 years ago. The concept Pharmacogentics began in the 1950s, nearly by chance, as a result of isolating genetic differences in metabolizing rugs. Numerous findings provided an early stimulus for the development of Pharmacogentics For example, the inheritance of phase I reaction impairment studied on Succinylcholine (Muscle Relaxant). Since the 1950s, novel technologies have been combined with a new genetic approach to decipher variation at person to person level. Pharmacogentics has been broadly applied in the study and treatment of cancers. A classical case of Pharamacogentics in oncology happened way back in 1988, when the Journal on Clinical Investigation reported the case of a 40-year-old woman being treated for breast cancer. The woman almost died from a standard done of chemothera [autic agent] since she possessed a genetic defect due to which she was unable to metabolize the drug. Pharmacogentics played a major role in understanding the cause and led to an entirely new approach to treatment. Till date, it is widely known that reaction to cancer treatment can very widely from patient from patient to patient. [1] Pharmacokinetic Variations Drug metabolism Metabolism usually converts drug to metabolites which are more water soluble and thus more easily excreted. It can also convert products into therapeutically active compounds and may even result in the formation of toxic metabolites. Pathway of drug metabolism is classified as:
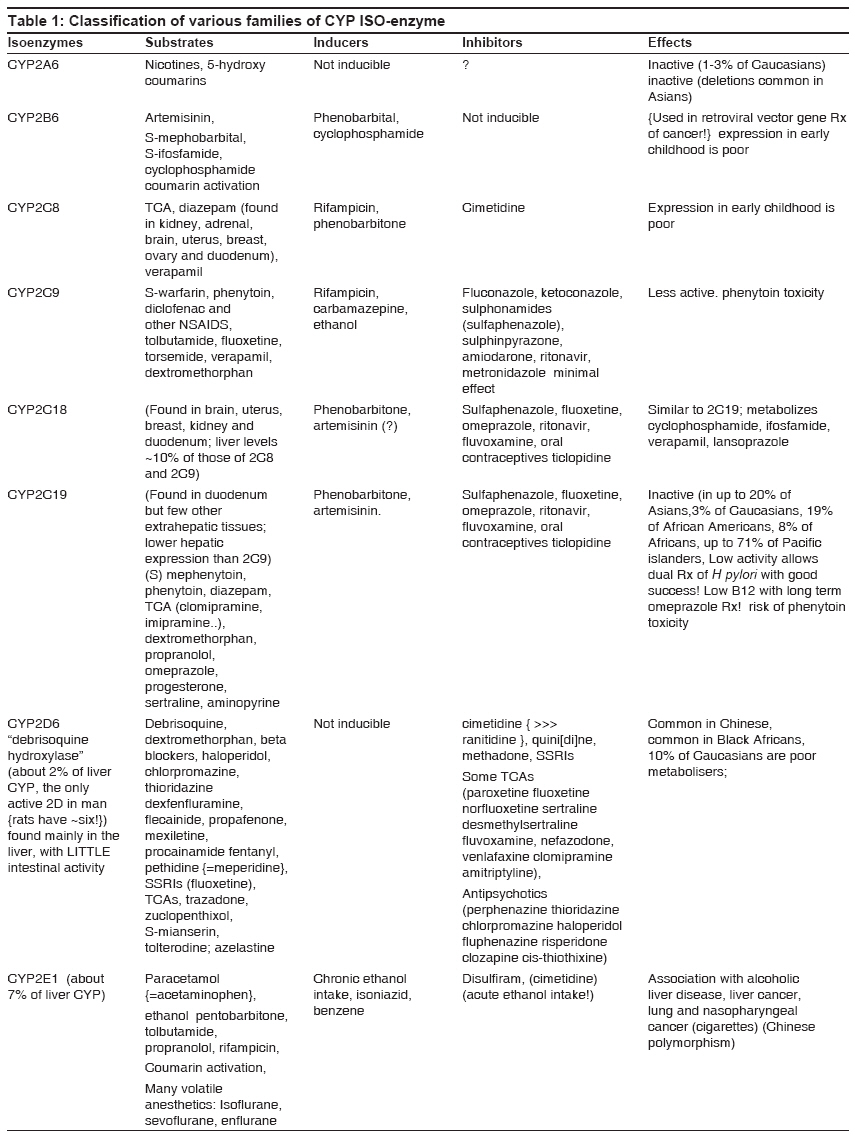
However, both the reactions often convert lipid soluble drugs into relatively more water- soluble metabolites. These fundamental reactions of drug metabolism are impacted by the individual′s genetic Information. Approximately 1 in 3500 white people code for an atypical form of enzyme butyl cholinesterase which is relatively unable to hydrolyze succinylcholine (muscle relaxant) thereby prolonging drug induced muscle paralysis and resultant apnoea. Similarly it has been observed that common genetic variations in phase II reactions e.g. Acetylation can result in objectionable differences in the half life and plasma Concentration of drugs metabolized by N-acetyltransferase e.g. Isoniazid, Hydralazine and Procainamide. These variations in Acetylation has clinical consequences. The Cytochrome P-450 enzyme, a super family of microsomal drug metabolizing enzymes, is the most important of enzymes which catalyze phase I drug metabolism reactions. One member of this family, CYP2D6 (cytochrome P-450 2D6), has been the most intensively studied and is the best example of Pharmacogenetic variation in drug metabolism. The CYP2D6 genetic polymorphism was originally discovered as a result of striking difference in the pharmacokinetics and therapeutic effects of drugs metabolized by this enzyme. Drugs as diverse as codeine, dextromethophan, metaprolol and tryptyline are all metabolized by this enzyme. CYP2D6 is needed to break down the drug and eliminate it. People who have low levels of enzymes metabolize drugs slowly and the drug will remain in the body for a longer period of time than it was metabolized quickly. Slow metabolizers are more likely to hace side effects. Moreover, people who produce low levels of CYP2D6 in liver will need smaller doses of drug hat are eliminated by this enzymes, while fast metabolizers i.e. people who have high levels of enzyme will need larger drug dose to get the same effect, by applying molecular genetic technique, 75 CYP2D6 alleles have been described. This CYP2D6 polymorphism is an excellent example of potential clinical implications of pharmacogentics. In some cases, the differences in drug responses can be correlated to ethnic background Noteworthy is the variation in Drug Metabolism enyzme in various ethnic groups [Table - 1]. [2] Pharmacodynamic Variations Drug response Genetic variations in drug target, e.g., receptors have a profound effect on drug efficacy. The response to 12- agonists is affected by genetic polymorphism of 12-adrenoceptor (coded by ADRB2 gene). Three single nucleotide polymorphism in ADBR2 have been associated with altered expression, down regulates or Coupling of the receptor in response to 12-receptor agonists. In some individuals it has been noticed that a dose up to 20 times greater than normal may be required to produce the desired anticoagulant effect by Warfarin. The reduced activity of Warfarin is attributed to a genetically controlled reduction in binding affinity of Warfarin receptor. [3] A life threatening malignant hyper thermis affects about one in 20,000 patients. This disorder causes a fatal elevation in body temp and is consequent to a hyper- metabolic response to a combination of a depolarizing muscle relaxant (SuccinylCholine) and a Potent Volatile inhalational General Anaesthetic (Halothane). The susceptibilty to the disorder (inherited in an autosomal dominant pattern) is due to mutation in the gene that encodes the ryanodine receptor (Calcium release channel). ACE-inhibitor improves symptoms of survival in case of heart failure in Caucasians as compared to African- Americans. This implies that a genetic screening of individuals might be allowed to apply this knowledge in clinical practice. Certain drugs act by binding to specific chemicals called receptors sites on the surface of our body within body cells. Variation in those genes that code for receptors means that same people may produce receptors that do not interact well with the drug, for example. Some people do not respond to the bronchodilator Salbutamol as they show genetic variation in the gene those codes for a receptor on surface of S.M cellular lining the bronchial airways. Drug Development A sound knowledge of the genetic make-up of an individual can be of importance in drug treatments trials. In Alzheimer disease which affects 25% of people in older age group of over 85, the gene associated is called APOE. This gene occurs in three forms known as E2, E3 and E4. All three have the same primary function to produce an essential protein called apoliprotein E is split of contain slightly different information this protein modifies the development of Alzheimer disease by interfering with the production of a brain cortex and the ceels deteriorate. The most common form of gene is E3. The E4 from gene is Supposed be associated with Alzheimer disease and the same is also distinctly involved in drug treatment for Alzheimer diseases. Individuals with Alzheimer disease who have E2 and E3 from of APOE gene respond well to the drug Tacrine (r), while those with E4 do not. [4] Ethical issues The idea of targeting certain groups within population can be a touching subject, no matter how well intentioned, as in the case of targeting sickle cell anaemia screening in early 1970′s to the American black population without appropriate knowledge. Such programs, if conceptualized, have to be carefully implemented to avoid a perception of stigma based or ethnicity. Moreover, questions might be raised on the assumptions that a person′s race can indicate their genetic profile for drug response since all the people belonging to a particular ethnic group will not have the same genetic variations. Consequently, genetic profiling may culminate into denial of treatment to a certain ethnic group race if a Pharmacogenetic test that could determine more precisely how a person′s reaction, was not available. Merits
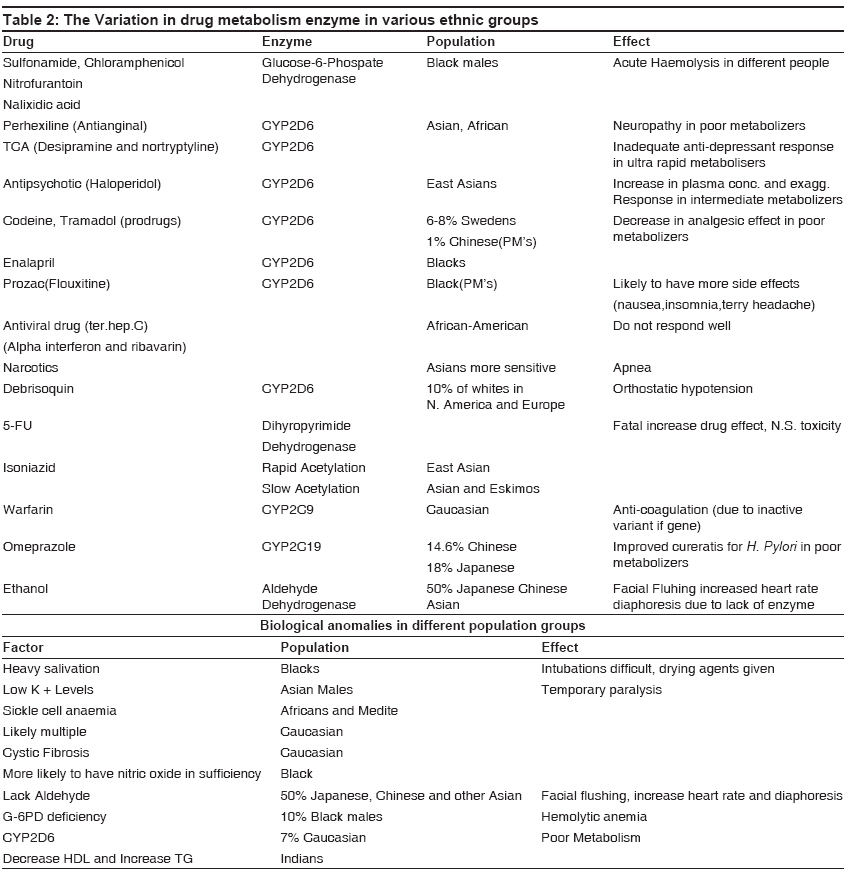
In some cases, the differences in drug responses can be correlated to ethnic background Noteworthy is the variation in drug metabolism enzyme in various ethnic groups [Table - 2]. [5] Conclusion The ramification of Pharmacogentics is the ability to screen potential adverse reactions. Technological advances in the way of human genome project (completed in April 2003) will finally allow us to tailor drug therapies to each patient and move beyond ′race′ as a crude indicator or genetic variations. Genetic finger printing of an individual is already practical. This can determine the presence of polymorphism in genes and an individualized care can be given in future. Studies to correlate DNA finger prints with data present in medical records about medical history and drug response can be undertaken. These studies will have a deep impact on the ways in which new drugs are developed and used. Such programs, if conceptualized, have to be carefully implemented to avoid a perception of stigma based or ethnicity. Moreover, questions might be raised on the assumptions that a person/race can indicate their genetic profile for drug response since all the people belonging to a particular ethnic group will not have the same genetic variations. Consequently, genetic profiling may culminate into denial of treatment to a certain ethnic group/race if a Pharmacogenetic test that could determine more precisely how a person reacts was not available. References
Copyright 2009 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg09019t2.jpg] [hg09019t1.jpg] |
| |||||||||

{kind=link}
{kind=link}