 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
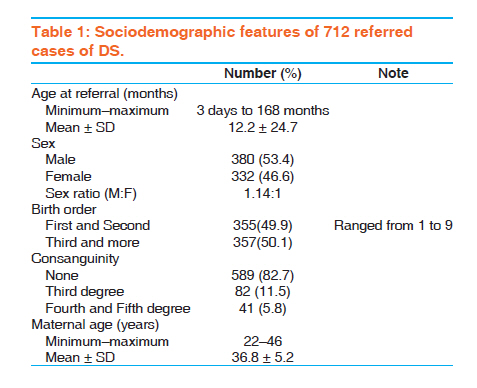
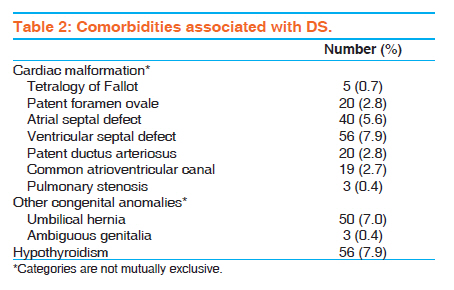
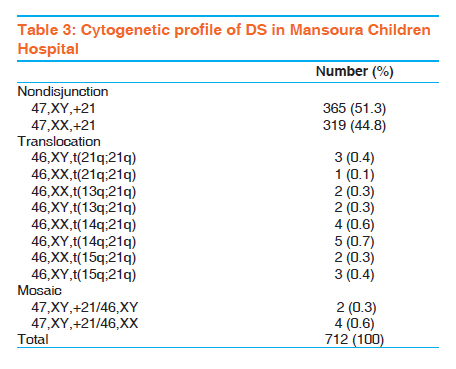
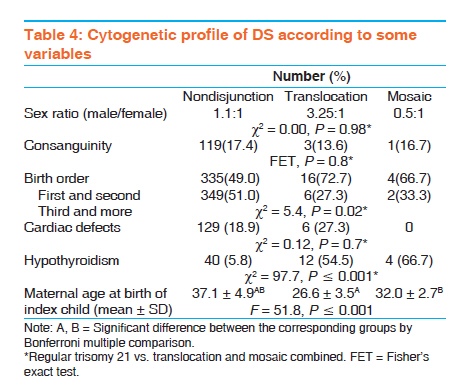
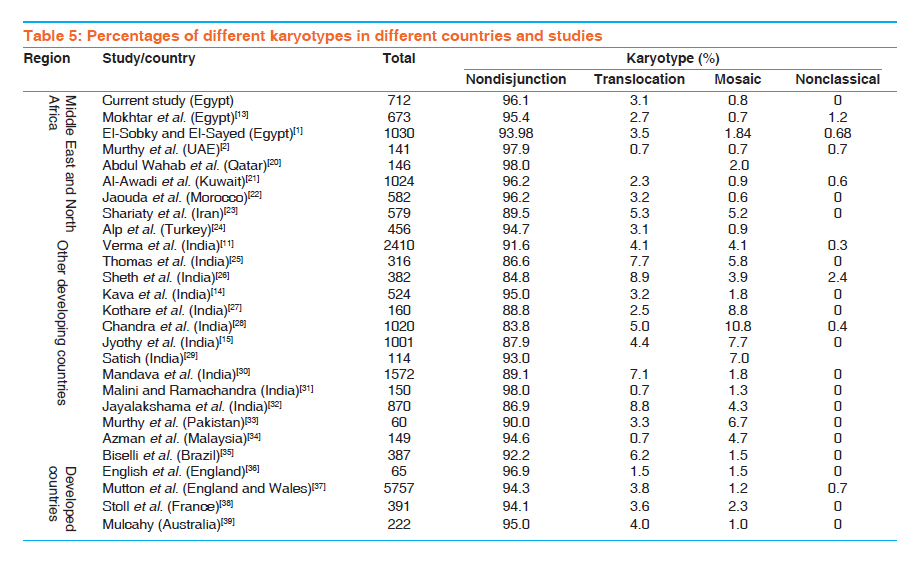
Indian Journal of Human Genetics, Vol. 17, No. 3, September-December, 2011, pp. 157-163 Original Article Cytogenetic and comorbidity profile of Down syndrome in Mansoura University Children's Hospital, Egypt Abdel-Hady El-Gilany1, Sohier Yahia2, Mohamed Shoker2, Faeza El-Dahtory3 1 Department of Public Health, Mansoura University Children's Hospital, Mansoura, Egypt Code Number: hg11035 DOI: 10.4103/0971-6866.92092 Abstract Background: Down syndrome (DS) is the most common chromosomal disorder. It has three chromosomal patterns. Keywords: Down syndrome, karyotypes, mosaic, nondisjunction, translocation Introduction Down syndrome (DS) is the most common chromosomal disorder. It is the single most common genetic cause of mental retardation and is thus of major socioeconomic concern. [1],[2] The overall incidence of DS worldwide is reported to be 1 per 600 to 1 per 800 live births. [3] In Egypt, the incidence of DS has been reported to be 1 per 1000 births. [4] There are several reports on the increased incidence of DS from different parts of the world, with respect to ethnicity and maternal age. [3],[5],[6],[7],[8] Governmental care of this syndrome has increased in the past few years. On the other hand, prenatal screening is still inaccessible to most families and almost all cases of DS were diagnosed postnatally. [1] DS can be caused by three types of chromosomal abnormalities: trisomy 21 (nondisjunction), translocation, or mosaicism. [9] Trisomy is characterized by the presence of three complete copies of chromosome 21, generally resulting from nondisjunction during maternal meiosis and is seen in about 95% of cases. [10] Translocations are attributed to 3-4% of the cases and mosaicism is reported in 1-2% of DS cases. These rates of cytogenetic abnormalities are described in basic literature, but specific studies reported variation in the cytogenetic pattern of the syndrome. [1],[11],[12],[13],[14],[15],[16] Cytogenetic diagnosis is important for the confirmation of the clinical diagnosis and for the determination of the risk of recurrence and thereby helping genetic counseling. This risk differs greatly between the cases as nondisjunction, and mosaicism rarely recur in siblings of people with DS; translocation may be recurrent, depending on the type of translocation. [9] DS is associated with a high risk of congenital heart diseases and other multiple malformations and/or various medical problems. [17] The association between thyroid dysfunction and DS is well recognized, but the natural history of this dysfunction is not known. [18] To the best of our knowledge, only two Egyptian studies were done in Alexandria [14] and Ain Shams [1] universities to describe the cytogenetic profile of DS and no studies were done in Mansoura. The aim of this study was to describe the cytogenetic pattern and associated comorbidity in DS in cases referred to the Genetic Unit of Mansoura University Children Hospital, Mansoura, Egypt. We compared our findings with those of previous local and international studies. Materials and Methods This is a retrospective record-based descriptive study conducted in the Genetic Unit of Mansoura University Children′s Hospital, Mansoura, Egypt. This is the only tertiary-care genetic unit in Dakahlia and nearby governorates. A total of 712 children with DS were confirmed by cytogenetic diagnoses during a 10-year period (from 2000 to 2009). Detailed background information of all patients was registered at the time of initial evaluation. All patients were subjected to full clinical, laboratory, and cardiac echo examination. The patient′s peripheral blood samples were used for cytogenetic diagnosis. Diagnosis of DS was based on the characteristic clinical features and confirmed by cytogenetic study for all cases. The data collected from medical records included sociodemographic characteristics of the child and his mother, comorbidity, and results of cytogenetic culture (katyotyping). Chromosomal culture was done according to the method described by Rooney and Czepulkowski. [19] One milliliter of sodium-heparinized whole blood was collected from each patient and control individual. A blood sample of 0.5 cm 3 from each patient and control individual was added to 5 cm 3 of a complete media containing Roswell Park Memorial Institute (RPMI) 1640, fetal calf serum (10%), phytohaemoagglutinin (PHA) (10 μg/ml), L-glutamate (2 mM), penicillin (200 unit/ml), and gentamicin (50 μg/ml). After 72 h of incubation at 37°C, colcemid was added (0.2 μg/ml). After 90 min, the cells were harvested by centrifugation (150 × g for 10 min). Then, 5 ml of 0.075 M KCl solution was added and mixed and incubated at 37°C for 90 min. After centrifugation (150 × g for 10 min), hypotonic supernatant was removed. Then, 5 cm 3 of cold, fresh fixative solution (3:1 methanol-acetic acid) was added dropwise to the cell pellet. Centrifugation was done afterward, and the supernatant was removed. These last two steps were repeated until a clear pellet was obtained. Finally, cells obtained were dropped on distinct slides. Staining with Giemsa was performed for some of the slides prepared from each patient. Fifty metaphases, each cultured on both the patients and the normal controls, were analyzed. Data were analyzed using the software SPSS, version 16 (SPSS Inc. Chicago ILL, USA). Quantitative variables were presented as mean and standard deviation. The analysis of variance test with Bonferroni multiple comparisons was used to compare maternal age at the birth of the index child between different karyotypes. Categorical variables were presented as the number and percentage, and chi square or Fisher′s exact test was used for comparison between different karyotypes, as appropriate. P ≤ 0.05 was considered statistically significant. Results A total of 15,903 cases were referred for consultation, and 712 (4.5%) cases were confirmed by cytogenetic study as DS during the decade 2000-2009. The mean age at referral was 12.2 months and the sex ratio was 1.14:1. About half of the cases were of first and second birth orders, and parental consanguinity was reported in 17.3% of the cases. The mean maternal age at the index pregnancy was 36.8 years [Table - 1]. [Table - 2] shows that about 19% of the cases had one or more cardiac anomalies and about 8% of the cases had hypothyroid. The abnormal karyotypes are listed in [Table - 3]. Nondisjunction was the most common type of abnormality, followed by translocation and lastly mosaic: 96.1, 3.1, and 0.8%, respectively. [Table - 4] shows that there is a marked excess of males in translocation and nondisjunction groups (sex ratios were 3.25 and 1.1, respectively, compared to a sex ratio of 0.5 in the mosaic group). However, this difference is statistically insignificant. Also, parental consanguinity and the presence of cardiac defects were not statistically significant. On the other hand, hypothyroidism was significantly more common in translocation and mosaic karyotypes than in the nondisjunction karyotypes. Lower birth orders (first and second) were significantly higher in the translocation and mosaic groups than in the nondisjunction group. Mothers are significantly older at birth of the index child in the nondisjunction group than those in the other two groups. [Table - 5] shows a comparison of the karyotyping pattern of the current study with the results of findings of previous local and international studies. Discussion The data reported in this study represent the first study on DS in Mansoura, Egypt. All cases were diagnosed postnatally. The age at referral ranged from 3 days after birth up to the age of 168 months, with a mean of 12.2 months. This may reflect low awareness of the family as well as health-care provider for early suspicion of affected newborns. Prenatal diagnosis of DS is not practiced in Egypt; this could be attributed to the lack of awareness, specific policy, and guidelines. A previous Egyptian study reported that most of DS cases were diagnosed postnatally and only 1.56% were detected prenatally mainly through amniocentesis and rarely through products of conception. In the same study, the age of referral ranged from 1 h after birth up to 30 years, with a median of 3 years. [1] An earlier study in England and Wales revealed that 37.8% of DS cases were diagnosed prenatally, 59.9% were diagnosed postnatally, and 2.3% were diagnosed among spontaneous miscarriage. In the same study, 94% of the postnatal referrals were within 10 days of birth, but the oldest child was referred at the age of 3 years. [37] Late referral of DS cases seems to be the norm in developing countries. The mean age at referral was 10.6 months in a Malaysian study [34] and 19.4 and 18.8 months in two Indian studies. [14],[29] In this study the overall sex ratio (male/female) was 1.14:1. Much excess of males was observed in translocation DS and an excess of females was observed in mosaic DS. The excess of males appears to be universal and was reported in all studies in different countries and the sex ratio ranged from 1.1:1 to 2.3:1. [1],[14],[20],[24],[26],[28],[29],[30],[32],[37] The referral pattern may influence the sex ratio as most of the studies were hospital based. However, in his meta-analysis of 55 publications on the sex ratio in DS, Kovaleva [40] concluded that the sex ratio was skewed toward an excess of males in the majority of studied populations, either in population with a high level of ascertainment (epidemiologic studies) or in selected groups. This phenomenon is not restricted to free trisomy 21 alone but appears in translocation cases. The genetic mechanisms of male predominance is explained by models for joint segregation of chromosome 21 and chromosome Y in spermatogenesis, and chromosome nondisjunction during the second meiotic division of oogenesis caused by Y chromosome-bearing spermatozoa. The birth order of children with DS ranged from 1 to 9. Overall, half of them were of first and second birth orders. This agrees with the previous studies from Egypt, Iran, and India. [1],[15],[23],[28] On the other hand, a study in UAE reported that a child with DS was mostly the last or second last child. [2] When children are stratified by karyotypes, we found that about two thirds of translocation and mosaic children were of first or second parity compared to about half of the nondisjunction children. There are controversial reports on the parity and risk of DS, but several studies suggest an increased risk with increasing parity. [41],[42],[43],[44],[45] One study reported that there is no increased risk with increased parity and gravidity after adjustment for age. [41] Another study suggested a trend toward an increasing risk of DS with the increased parity in both younger and older mothers. [45],[46] About 17% of the patients with DS were products of consanguineous marriages. The proportion of consanguineous marriage did not differ according to karyotype. Previous studies in Egypt and Iran reported parental consanguinity in 12 and 10.4%, respectively, among children with DS. Maternal age at birth of all studied DS children ranged from 22 to 46 years, with a mean of 36.8 years. Older maternal ages were reported in previous studies in different countries. [1],[14],[22],[24],[34],[37] However, other studies reported a much younger maternal age. [14],[23],[26],[27],[28] Mothers of children with nondisjunction DS are significantly older than those of translocation and mosaic children (37.1 years vs. 26.6 and 32.0 years, respectively). This is in agreement with previous findings. [1],[14],[24],[28],[37] A previous Egyptian study reported that all mothers of cases of translocation DS were under 35 years, in contrast to mothers of nondisjunction cases in which 41.5% were above 35 years. [1] Congenital heart diseases were diagnosed in 18.9% of DS cases with no significant difference according to the karyotype pattern. The most common cardiac defects were ventricular septal defect (7.9%) and atrial septal defect (5.6%). Congenital cardiac defects were reported to be the most frequent congenital anomalies associated with DS up to 59% in a previous study. [29] Another study reported that 25.1, 27.5, and 5.5% of nondisjunction, translocation, and mosaic karyotypes had congenital heart disease. [28] Kava et al. [14] reported that congenital heart diseases in 18.3% DS with ventricular septal defect, tetralogy of Fallot, and atrial septal defects were the most frequent. The association between thyroid dysfunction and DS is well recognized. We found that 7.9% of the DS children had hypothyroid. Hypothyroidism was significantly lower in nondisjunction (5.8%) than in translocation (54.5%) and mosaic (66.7%) children. Much higher rates of thyroid dysfunction were reported in previous studies. Satish [29] found that 14.9% of the DS cases had thyroid dysfunction. Cutler et al. [40] found that 61.2% of the DS children had congenital hypothyroidism. They commented that transient elevations of thyroid-stimulating hormone (TSH) were common in children with DS whether or not TSH values were initially normal or elevated. Gibson et al. [18] in his longitudinal study concluded that hypothyroidism in DS should not be overdiagnosed. Knowledge of isolated raised TSH (IR-TSH) and its frequent self-limiting natural history needs dissemination. Treatment and frequent retesting of IR-TSH is not indicated. [1],[23] The current study revealed that the frequency of nondisjunction, translocation, and mosaic was 96.1, 3.1, and 0.8%, respectively. The proportion of nondisjunction in other local and international studies ranged from 83.8 to 98.0%. [1],[2],[11],[13],[14],[15],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30],[31],[32],[33],[34],[35],[36],[37],[38],[39] In all studies done in the Middle East and North African countries, this proportion was above 94%, [1],[2],[13],[20],[21],[22],[24] except in the Iranian study (89.5%). [23] In the 12 Indian studies, there was marked variability in the proportion of nondisjunction, ranging from 84.8 to 98.0%. [11],[14],[15],[25],[26],[27],[28],[29],[30],[31],[32] Previous studies have reported that the frequency of DS translocation varied from 0.7 to 8.9% and the frequency of DS mosaic varied from 0.7 to 10.8%. [1],[2],[11],[13],[14],[15],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30],[31],[32] A general observation in all studies is that the frequency of translocation and mosaicism was very much lower than the frequency of nondisjunction. This could be attributed to the high fertility trends toward reproduction even at an advanced maternal age. It has been reported that translocation may arise as a sporadic event (de novo) or may be transmitted by a carrier parent (familial). [13] Nondisjunction, translocation, and mosaicism are the classical anomalies of DS. In the past decades, nonclassical types of chromosomal anomalies (whether numerical or structural) have been reported in many DS studies, with frequency ranging from 0.3 to 1.2%; [1],[11],[13],[21],[28],[37] only one study reported a higher frequency (2.4%) of nonclassical DS. [26] The identification of the type of chromosomal anomalies in DS could enable care givers accurately counsel the parents regarding the recurrence risk and available options. Early case detection is important for early intervention to the patients and their families by genetic counseling and helping in planning care to these children to improve their life′s quality. It is important to educate women at high risk of recurrence (e.g., advanced maternal age) to go for screening during pregnancy. The concept of preventive genetics should be reinforced with the national policy targeting both health professionals and the general public to offer prenatal screening for at-risk women. Routine cardiac echo/color Doppler examination and neonatal and sequential thyroid screening of DS cases are warranted. A wide-scale national community-based survey together with DS registry could help in estimating the size of the problem and in estimating future needs of these physically challenged children. References
Copyright 2011 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg11035t5.jpg] [hg11035t4.jpg] [hg11035t2.jpg] [hg11035t3.jpg] [hg11035t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}